East Asian Arch Psychiatry 2011;21:123-127
ORIGINAL ARTICLE
梁德瑜、梁国辉、林翠华
Dr Grace Tak-Yu Leung, MRCPsych, FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, Tai Po Hospital, Hong Kong SAR, China.
Dr Kwok-Fai Leung, PDOT, MPhil, Department of Occupational Therapy, Queen Elizabeth Hospital, Hong Kong SAR, China.
Prof Linda Chiu-Wa Lam, MD, FRCPsych, Department of Psychiatry, The Chinese University of Hong Kong, Hong Kong SAR, China.
Address for correspondence: Dr Grace Tak-Yu Leung, Department of Psychiatry, Tai Po Hospital, Tai Po, New Territories, Hong Kong SAR, China.
Tel: (852) 2607 6111; Fax: (852) 2667 1255; Email: schroederleung@yahoo.com.hk
Submitted: 30 December 2010; Accepted: 22 March 2011
Abstract
Objectives: To develop a classification to describe leisure activities of elderly Hong Kong Chinese based on the functions fulfilled, namely: intellectual, physical, social, and recreational.
Methods: A focus group comprising care-for-the-elderly professionals was invited to identify leisure activities commonly practised by elderly Chinese in Hong Kong. An independent panel of occupational therapists in the field of geriatrics and psychiatry was invited to classify the activities into physical, intellectual, social, and recreational categories based on their professional opinion in the context of local practice. The classification was then validated against the opinions of a non-depressed elderly convenience sample with relatively preserved cognition.
Results: A total of 33 types of activities were identified, of which 13 were classified as intellectual, 8 as social, 9 as recreational, and 3 as physical. The 3 types of physical activities (mind-body exercise, strenuous aerobic exercise, and stretching and toning exercise) were further divided into different subtypes.
Conclusions: An easy-to-understand classification of late-life leisure activities among Chinese has been developed.
Key words: Aged; Hong Kong; Leisure activities / classification
摘要
目的:开发针对香港华籍长者休閒活动系统,以智力、体力、社交和消遣分类。
方法:研究邀请老人护理专业人员组成焦点小组,确认香港华籍长者经常进行的休閒活动,并透过由老人科和精神科职业治疗师成立的独立小组,根据他们的在职经验把这些休閒活动分为体力、智力、社交和消遣类别。然後以便利抽样方法选出非抑鬱症长者,以他们对此分类的观点作对照和验證。
结果:研究确立33项休閒活动,当中13项为智力活动、8项属社交类别、9项属消遣,以及3项体力活动;这3项体力活动(身心锻炼、带氧运动和舒展运动)再被细分为不同类型的活动。
结论:这项研究开发了针对香港华籍长者简易休閒活动参与分类系统。
关键词:长者、香港、休閒活动/分类
Introduction
Leisure activities could be broadly defined as those in which individuals engage for enjoyment or well-being, which are independent of work or the activities of daily living.1 They have undoubted value in life-career development and individual well-being. In recent years, there has been an abundance of clinical and neurobiological studies examining the modulating effects of leisure activity participation on several outcomes, including mental health and cognitive function.1-7 A community-based, cross-sectional study conducted in Brazil showed a negative association between participation in leisure activities and several anxiety or depression symptoms among women reporting no job satisfaction and low family income.2 A population-based survey conducted in Australian adolescents demonstrated that leisure participation has a significant positive relationship with mental health, and positively influences self-efficacy, competence, and global self-worth.3 Studies from different parts of the world support the association between participation in late-life leisure activities and cognitive function, as well as the idea that late-life leisure activity participation protects against cognitive decline and dementia.1,4-7 Yet, literature review reveals a scarcity of studies on the classification system for leisure activities. The interpretation, application, and communication of clinical leisure research findings are usually hampered by the lack of any empirically based and comprehensive organisational scheme for such activities.
There were 5 proposed approaches to the development of a classification system for leisure activities, as reviewed and developed in a previous study.8 Overs et al9 classified more than 800 leisure activities into 9 groups by relating information about such activities to available community vocational opportunities, patterned after the Dictionary of Occupational Titles.9 Although neither empirically based nor validated, this system is very comprehensive. Holmberg et al10 proposed a taxonomy of leisure activities by assigning 2-letter Holland codes to 760 leisure activities on the basis of counsellors’ judgements of the comparability of occupations and leisure activities.10 This taxonomy has not been tested empirically. The third approach is to factor analyse the frequency of participation in leisure activities11-14; however, this approach could not reflect the nature of these activities to enable comparisons. A fourth approach was proposed by Allen15 who related 212 undergraduate students’ interests in 51 leisure activities to their scores on the Personality Research Form-E. This had been criticised in that the data were confounded by the stereotypic impressions on the activities of interviewees in the activities they had not actually participated in. The fifth approach was based on information about the psychological needs gratified by participation in a specific leisure activity.8 From this study, 12 leisure activity clusters were identified (with 1 group judged to be a residual), namely: agency, novelty, belongingness, service, sensual enjoyment, cognitive stimulation, self-expression, creativity, competition, vicarious competition, and relaxation. This classification was produced empirically from a large number of participants, yet the psychological terms used may not be readily understood by lay individuals, and a classification based on these 12 activity clusters may be difficult to adopt in studies and challenging to promote in the community.
There are 3 reasons for the lack of literature on this subject. First, although the concept of leisure activities is intuitively accessible, in practice such activities are difficult to standardise, classify, and measure. Various theoretical definitions and operationalisations of activity engagement have been used in previous studies and have been categorised arbitrarily in several ways. Second, leisure activities may vary across different eras, age-groups, geographical, cultural and socio-economic contexts. Thus, any classification needs to be tailor-made for a certain population of a region and having a given ethnicity. Third, this topic does not appear to be clinically crucial.
Researchers are generally unable to agree on how the concept of leisure activities should be defined or measured because of its complexity and diversity. From a statistical perspective, the definition of the construct of leisure activities can be determined by the instrument used to categorise and measure it. Subsequently, the construct may be conceptualised and hence categorised in terms of functions fulfilled by participation in each activity. We believe that each of the leisure activities serves 1 or more functions like cognitive stimulation, physical exercise, socialisation, and provision of entertainment. These functions may also be associated with the therapeutic benefits of leisure activities. Taking this approach in exploring such activities may be a key to understand more about how leisure activities contribute to well-being. In fact, this concept has been widely adopted in previous clinical studies, yet has not been validated empirically. Categorisation of leisure activities based on their functions is also readily understood by people of different backgrounds.
The significance of a classification of leisure activities lies in the need to communicate among researchers and also to convey messages to the individuals in the community trying to promote leisure activity participation as an intervention for diverse purposes. For example, they may focus on maintenance of cognitive function and overall health in older adults. An easy-to-understand and comprehensive categorisation in simple terms is of particular importance in older persons, especially those with lower education levels or mild cognitive impairment.
The objective of the present study was to develop a classification of leisure activities among elderly Chinese, based on the functions fulfilled, namely, intellectual, physical, social, and recreational.
Methods
The participants consisted of a focus group, an elderly convenience sample, and an expert panel. The focus group was comprised of care-for-the-elderly professionals, including: psychogeriatricians, a social worker, a clinical psychologist, occupational therapists, and physiotherapists. This group aimed at identifying leisure activities which were commonly practised by elderly Chinese in Hong Kong. After thorough discussion, 33 types of activities were identified. The independent panel of occupational therapists in the field of geriatrics and psychiatry was invited to classify the activities into physical, intellectual, social, and recreational categories, based on their professional opinion in the context of local practice. The classification was then validated against the opinions of the elderly convenience sample as described below.
The convenience sample of community-dwelling elderly people aged ≥ 60 years was approached through the elderly community activities and conduction of a community survey. Inclusion criteria were: (1) having a Cantonese Mini-Mental State Examination (CMMSE)16 score of ≥ 25; and (2) having a Cantonese-version Geriatric Depression Scale (CGDS)17 score of ≤ 8. These cut-off scores were adopted to ensure recruitment of non-depressed elderly people with relatively well-preserved cognitive function.18,19 Consent from each of the participant was obtained. These elderly participants were asked to assign a physical, intellectual, social, and recreational component score to each activity in which they had participated, based on their evaluations of how helpful the activity was in fulfilling the corresponding functions using a 4-point scale (0 = not helpful; 1 = of little help; 2 = of some help; and 3 = of a lot of help). These functions were defined through discussion among experienced psychogeriatricians and an occupational therapist interested in this field. This entailed: (1) intellectual component scores (how helpful the activity was in training memory and thinking); (2) physical component scores (how helpful the activity was in training physical strength and in exercising muscles); (3) social component scores (how helpful the activity was in maintaining social contact and communication with others); and (4) recreational component scores (how helpful the activity was in providing entertainment while lacking the above 3 functions).
After these activities had been categorised according to the classification determined by the expert panel, a mean
Table 1. Scores of activity components in each activity category.
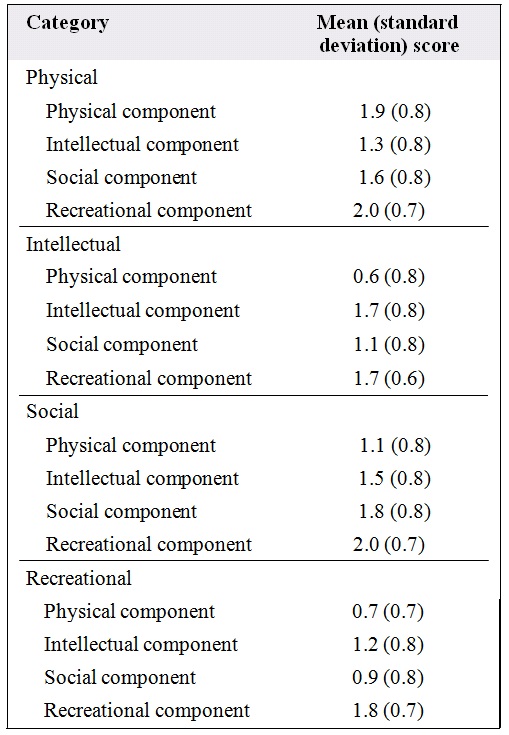
for each component score in each activity category was computed, such that each had 4 mean component scores. It was presumed that if the results from the expert panel and from the elderly sample were consistent, the corresponding mean component score of each category would be the highest.
Results
A total of 75 eligible elderly participants were recruited. Among these, 55 were female (73%) and 20 were male (27%). The mean (standard deviation [SD]) age was 75 (7) years and the mean (SD) duration of education was 4.7 (4.3) years. The mean (SD) CMMSE score was 27.5 (1.6) and the mean (SD) CGDS score was 1.9 (1.9).
The mean component scores of the 4 categories are shown in Table 1. Among all of the categories, the mean recreational component score was the highest, and the corresponding mean component scores of physical, intellectual, and social categories were the second highest. This is because the elderly sample generally assigned high recreational component scores to all of the activities. If the recreational component scores were excluded from the analyses, the corresponding mean component score in each of the physical, intellectual, and social categories was significantly higher than the other scores when compared by analysis of variance and post-hoc tests (Table 2). This showed that the results from the expert panel and the elderly sample were consistent overall.
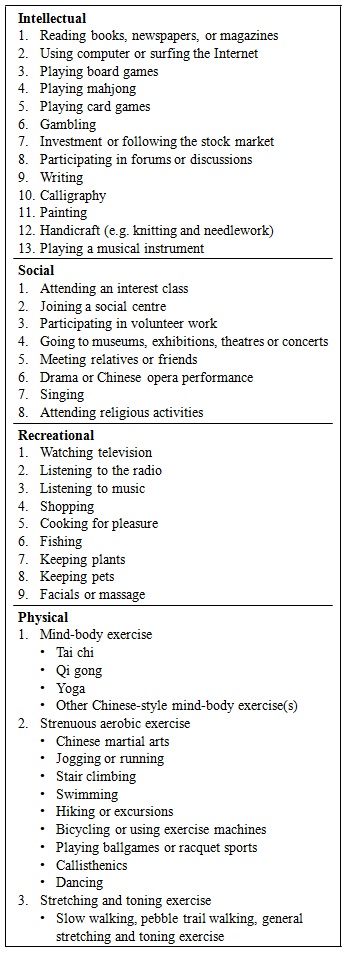
The classification is shown in Table 3. There were 13 types of intellectual activities, 8 types of social activities, 9 types of recreational activities, and 3 types of physical activities. The 3 types of physical activities (mind-body exercise, strenuous aerobic exercise, and stretching and toning exercise) were further divided into different subtypes.
Table 2. Comparison of corresponding component and other component scores after exclusion of recreational component scores.*
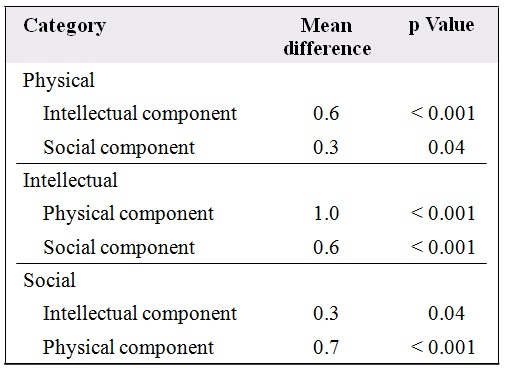
* Analysis of variance and post-hoc tests were performed.
Table 3. Classification of leisure activities.
Discussion
A classification of common late-life leisure activities among Hong Kong elderly Chinese has been developed with the help of community-dwelling elderly and a group of professionals. Notably, the activities list could not be exhaustive as more and more choices are made available to the elderly. Nor is the categorisation mutually exclusive, as some activities, such as playing mahjong, encompassed more than 1 function. The system aimed to prioritise the different domains for each activity, and had to be easy to understand and adopt in the design of further studies and intervention programmes. The content validity of the classification was ascertained by discussion and review of the content by experts on elderly care from different disciplines. The construct validity was partially reflected by the convergent validity, in that the results from the occupational therapists and the non-demented elderly convenience sample yielded a strong correlation.
The elderly convenience sample generally assigned high recreational component scores to all of the activities, because in Chinese the meaning and interpretation of the word ‘leisure’ is very similar to that of ‘recreational’. When this factor was excluded, the results showed that the opinions from the experts and the elderly were consistent. One limitation in our study was the relatively small sample size with a female predominance. This could be explained by the fact that the eligibility criteria of CMMSE score of ≥ 25 excluded a considerable number of elderly who had a below-mean CMMSE score19 and that females were more active participants in community activities.
Among different subtypes of activities, some are particularly popular in the Chinese elderly community compared to their Caucasian counterparts. Mahjong is a traditional Chinese game that involves several cognitive domains like attention, memory, calculation, executive function, and social interaction with other players. There are some variations of terms and regulations in playing the game in different provinces, and elderly from the same native province may like to play together as a social gathering. While mind-body exercise like yoga is usually an activity of young age-groups in the western world, Chinese- style mind-body exercises like Tai chi and Qi gong are commonly practised by local elderly as a kind of morning exercise.
The pattern of elderly leisure activities reflects some characteristics of lifestyle in Hong Kong. As an important financial centre, investment is very popular. Many older adults start their career in following the stock market after retirement, even though they knew little about investment when they were young. As computers are readily accessible in elderly social centres or at home, those with relatively preserved cognition may be able to learn simple skills like web surfing even if they had not used computers earlier. Since the majority of elderly live in small public housing apartments, ‘keeping plants’ may mean taking care of a few potted plants. This has a very different meaning to ‘gardening’ or ‘yard work’ in places with more spacious living environments, the latter activity being more physically and cognitively demanding. In our locality, pebble trail walking is common in the middle-aged and elderly, and reflexology as an alternative treatment is also quite popular in these age-groups.
A mounting number of studies have demonstrated the potential benefits of low-risk, low-cost leisure activities for the elderly. Notably, the therapeutic elements of leisure activities in mental health are becoming a global and cross- disciplinary discussion. An empirically based and user- friendly classification system of leisure activities therefore has an important place in research, mental health and elderly services. A valid categorisation improves the quality of data collection, facilitates subsequent analysis, and enhances the accuracy of interpretation. This classification should prove valuable in developing a balanced and enriching programme of leisure services in a variety of settings. In addition, it has implications for the interchange of leisure activities, because activities in the same group have similar functions. As an individual has to change the leisure activities due to various reasons, functionally equivalent activities can replace the current options.
The development of the leisure activity classification system proposed herein only represents groundwork for leisure research and delivery of services in the elderly. The classification may be generalised to other Chinese communities. However, further studies with a larger sample are needed to refine and consolidate our findings. The distinct benefits of late-life leisure activity participation have to be explored in longer-term clinical trials. Hopefully, this classification may provide a preliminary organisational scheme that allows greater precision in testing hypotheses about leisure activities, and create a synergism with current rigorous research in this area.
References
- Verghese J, LeValley A, Derby C, Kuslansky G, Katz M, Hall C, et al. Leisure activities and the risk of amnestic mild cognitive impairment in the elderly. Neurology 2006;66:821-7.
- Pondé MP, Santana VS. Participation in leisure activities: is it a protective factor for women’s mental health? J Leisure Res 2000;32:457-72.
- Passmore A. The occupation of leisure: three typologies and their influence on mental health in adolescence. OTJR: Occupation, Participation and Health 2003;23:76-81.
- Verghese J, Lipton RB, Katz MJ, Hall CB, Derby CA, Kuslansky G, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med 2003;348:2508-16.
- Wang JY, Zhou DH, Li J, Zhang M, Deng J, Tang M, et al. Leisure activity and risk of cognitive impairment: the Chongqing aging study. Neurology 2006;66:911-3.
- Wilson RS, Bennett DA, Bienias JL, Mendes de Leon CF, Morris MC, Evans DA. Cognitive activity and cognitive decline in a biracial community population. Neurology 2003;61:812-6.
- Wilson RS, Scherr PA, Schneider JA, Tang Y, Bennett DA. Relation of cognitive activity to risk of developing Alzheimer disease. Neurology 2007;69:1911-20.
- Tinsley HE, Eldredge BD. Psychological benefits of leisure participation: a taxonomy of leisure activities based on their need- gratifying properties. J Couns Psychol 1995;42:123-32.
- Overs RP, Taylor S, Adkins C. Avocational counselling manual. Washington DC: Hawkins & Associates; 1977.
- Holmberg K, Rosen D, Holland JL. The leisure activities finder. Odessa, Florida: Psychological Assessment Resources; 1990.
- 1 Ditton RB, Goodale TL, Johnsen PK. A cluster analysis of activity, frequency, and environment variables to identify water-based recreation types. J Leis Res 1975;7:282-95.
- Gudykunst WB, Morra JA, Kantor WI, Parker HA. Dimensions of leisure activities: a factor analytic study in New England. J Leis Res 1981;13:28-42.
- Kremer Y, Harpaz I. Leisure patterns among retired workers: spillover or compensatory trends. J Vocat Behav 1982;21:183-95.
- Yu J. The empirical development of typology for describing leisure behaviour on the basis of participation patterns. J Leis Res 1980;12:309-20.
- Allen LR. The relationship between Murray’s personality needs and leisure interests. J Leis Res 1982;14:63-76.
- Chiu HF, Lee HC, Chung D, Kwong PK. Reliability and validity of the Cantonese version of the Mini-Mental State Examination: a preliminary study. Journal of Hong Kong College of Psychiatrists 1994;4(Suppl 2):S25-28.
- Lee HC, Chiu HF, Wing YK, Kwong PK, Leung CM, Chung DW. The GDS short form as a screening test for the Chinese elderly: a preliminary study. Clin Gerontol 1993;14:37-41.
- Chiu HF, Lam LC, Chi I, Leung T, Li SW, Law WT, et al. Prevalence of dementia in Chinese elderly in Hong Kong. Neurology 1998;50:1002- 9.
- Lam LC, Tam CW, Lui VW, Chan WC, Chan SS, Wong S, et al. Prevalence of very mild and mild dementia in community-dwelling older Chinese people in Hong Kong. Int Psychogeriatr 2008;20:135- 48.