East Asian Arch Psychiatry 2013;23:102-8
THEME PAPER
Ms Ada Wai-Tung Fung, MSc, Department of Psychiatry, Tai Po Hospital, Hong Kong SAR.
Prof. Linda Chiu-Wa Lam, MD, FRCPsych, FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, Tai Po Hospital, Hong Kong SAR.
Address for correspondence: Ms Ada Wai-Tung Fung, Department of Psychiatry, Tai Po Hospital, 9 Chuen On Road, Tai Po, New Territories, Hong Kong SAR.
Tel: (852) 2607 6045; Fax: (852) 2667 5464; email: ada_fung@cuhk.edu.hk
Submitted: 24 April 2013; Accepted: 2 July 2013
Abstract
Objective: This cross-sectional study aimed to explore the association between late-life spiritual activity participation and cognitive function in older Chinese adults in Hong Kong.
Methods: Participants aged 60 years or older without clinical dementia or major psychiatric disorders were recruited. Dementia severity and global cognitive function were assessed using the Clinical Dementia Rating and Cantonese version of the Mini-Mental State Examination, respectively. Cognitive performance was measured using 10-minute delayed recall, the Category Verbal Fluency Test, Visual Aural Digit Span Test, and Modified Card Sorting Test. Psychological status was assessed using the Chinese version of the Purpose in Life scale. Activities participated in were categorised into 6 domains of physical, cognitive, social, prosocial, spiritual, and recreational activities.
Results: A total of 380 participants were enrolled. Bivariate correlation showed that the composite score of cognitive function was positively correlated with aerobic exercise (r = 0.14; p = 0.01), cognitive activity (r = 0.30; p < 0.001), and spiritual activity (r = 0.16; p = 0.002). Multiple linear regression suggested that frequent participation in cognitive activity (B = 0.87, beta = 0.22; 95% confidence interval [CI] = 0.52-1.25 and p < 0.001) and spiritual activity (B = 0.45, beta = 0.11; 95% CI = 0.13-0.76 and p = 0.01) were associated with better cognitive function after controlling for age and years of education.
Conclusion: Engagement in spiritual activity may benefit cognitive function in old age. Longitudinal studies are recommended to further examine the causal relationship of spiritual activity and cognitive function.
Key words: Aged; Cognition; Life style; Spirituality
摘要
目的:本横断面研究旨在探讨香港华籍长者参与晚年灵性健康活动与认知功能的相关性。
方法:纳入无临床脑退化或精神疾病的60岁或以上长者,以临床失智评分量表和粤语版简易精神状态量表分别评估他们的脑退化重度和总体认知功能,和进行10分钟延迟回忆、口语流畅、视觉听力数字广度和改良版卡片分类测验以测试他们的认知表现,并以生命目的量表中文版评估他们的心理状态。他们参与的活动涵盖6个範畴,包括体力、认知、社会、利社会、灵性健康和文娱活动。
结果:研究纳入了380名参与者。二变量相关分析显示,认知功能综合评分与有氧运动(r = 0.14;p = 0.01)、认知活动(r = 0.30;p < 0.001)和灵性健康活动呈正相关(r = 0.16; p = 0 . 0 0 2 ) 。 多 元 线 性 回 归 分 析 则 显 示 , 在 年 龄 和 教 育 因 素 控 制 下 , 频 繁 参 与 认 知 活 动 (B = 0.87,β = 0.22;95%置信区间 = 0.52-1.25,p < 0.001)和灵性健康活动(B = 0.45,β = 0.11,95%置信区间 = 0.13-0.76,p = 0.01)有助改善认知功能。
结论:参与灵性健康活动或有利改善老年认知功能,建议进一步纵向研究灵性健康活动和认知功能的因果关係。
关键词:长者、认知、生活方式、灵性
Introduction
Population ageing is taking place worldwide. According to the United Nation Population Division, the proportion of people aged 60 years or older has increased from 11% (645,546) in 2003 to 13.1% (955,243) in 2013, and is projected to increase to 25% in 2050.1 This growth in population ageing is most rapid in the Asia Pacific region. Due to the rapid growth of the ageing population, researchers are interested in exploring health and psychological factors associated with cognitive function in old age.2-5 Lifestyle cognitive activities are reportedly beneficial for cognition function.6-9 Cross-sectional association for a high level of participation in cognitive activities with reduced risk of developing dementia and mild cognitive impairment has been reported.10,11 A study found that people who do crossword puzzles frequently are more likely to delay cognitive decline.12
Apart from cognitive activity, other lifestyle activities may also modulate brain and cognitive function. Epidemiological studies of the effect of physical activity on cognition demonstrated an inverse relationship between physical activity level and cognitive decline.4,13-15 A study reported that the incidence rate for Alzheimer’s disease (AD) was higher for individuals who exercised fewer than 3 times per week than for those who exercised more frequently.15 Findings from randomised controlled trials on the effect of physical exercise on cognition also reported cognitive improvement.16,17
The Nun study reported that lifestyle factors significantly influenced clinical manifestations of AD.18 While the result could be explained from a biological perspective, other modifiable lifestyle factors such as an active spiritual life may also contribute. However, there are very few studies exploring the effects of spiritual activity on cognition in old age. Two recent studies showed that engaging elderly people in religious activity reduced cognitive decline and helped to relieve depressive symptoms.19,20 A cross-sectional study found that long- term meditators have better cognitive function than non- meditators.21
To better understand how spiritual activities are associated with cognitive function, purpose in life in relation to cognitive function has been investigated. Spiritual activity enables a person to look into the meaning of life, and may be associated with reduced mood disturbance. Previous findings suggested that motivation to search for spiritual experience was associated with a greater sense of purpose in life.22-24 A study by Boyle et al25 found that expression of a purpose in life is associated with delayed decline in cognitive function. Several studies have also demonstrated a positive relationship between participation in spiritual activity and subjective well-being.26,27 Krause28 found that religious participation was related to subjective well-being among elderly people. This study aimed to examine the association between participation in spiritual activity and cognitive function in older Chinese adults in Hong Kong. The hypotheses were that a greater level of spiritual activity in later life is associated with positive purpose in life and that spiritual activity in later life is associated with better cognitive function.
Methods
Participants
The study participants were community-dwelling elderly people (aged ≥ 60 years) in Hong Kong. Participants diagnosed with clinical dementia or psychiatric illnesses were excluded. Interviews were conducted either at the participant’s home or in Tai Po Hospital, Hong Kong, according to their preference. Informed consent was obtained before the interview began. Global cognition, lifestyle, and demographic data were collected.
Assessments
Global Cognitive Function
The Clinical Dementia Rating (CDR)29 was used to ascertain dementia severity. The Cantonese version of the Mini-Mental State Examination (CMMSE)30 was used to assess global cognition, with a range of score from 0 to 30. Cognitive performance was measured by 10-minute delayed recall, the Category Verbal Fluency Test,31 Visual Aural Digit Span Test, and Modified Card Sorting Test.32
To obtain a composite score for cognitive function, raw scores for each of the cognitive tests were converted to z-scores. The z-scores were summed to obtain a composite score of cognitive function, with a higher score indicating better cognitive function.
Measurement of Leisure Activities
Leisure activities are categorised into 6 different domains. The activity classification was adapted from the activity questionnaire designed for older Chinese adults in Hong Kong.33 The original classification consisted of 4 activity domains of physical, cognitive, social, and recreational activities. After revision, we extracted prosocial activity and spiritual activity from the social activity domain, resulting in 6 domains for the new activity classification: physical activity (including mind-body exercise, strenuous exercise, stretching and toning exercises), cognitive activity, social activity, prosocial activity, spiritual activity, and recreational activity. The modified classification of leisure activities is shown in the Appendix. Frequency of leisure activity participation was calculated from the number of times per week and the duration on each occasion of each activity participated in during the previous year. The number of times per week of activity was multiplied by the duration (in minutes) to produce a weekly estimate of activity level.
Psychological Measurement
The Chinese version of the Purpose in Life scale was adopted to measure the extent to which respondents perceive meaning and purpose in their lives.34,35 The test is a 20-item self-report attitude scale, and each item is rated on a 7-point scale ranging from 1 (low purpose) to 7 (high purpose). The score ranges from 20 to 140, with a higher score indicating a greater sense of purpose in life.36
Potential Confounders
Socio-demographic data of age, sex, education, marital status, socio-economic status, and occupational status were obtained. Severity of physical and psychiatric illnesses was assessed using the Cumulative Illness Rating Scale.37 Depression was defined according to the ICD-10 criteria38 of persistent sadness and / or loss of interest and fatigue lasting for 2 weeks or more in the previous month. Severity of depression was measured by the depression section of the Clinical Interview Schedule–Revised, the score of which ranged from 0 to 4. A higher score indicated more frequent and severe symptoms.39
Data Analysis
Variables for normality were examined, and log transformation was done for those exhibiting a high level of skewness. Bivariate correlation was conducted to explore the correlations between cognitive score and frequency of engaging in different activities. Linear regression was performed to evaluate the association of participation in different leisure activities and cognitive function. Potentially confounding variables included in the regression analysis were age and years of education. Data analysis was performed using the Statistical Package for the Social Sciences Windows version 20.0 (SPSS Inc., Chicago [IL], US). Statistical significance was defined as p < 0.05.
Results
Demographic Characteristics
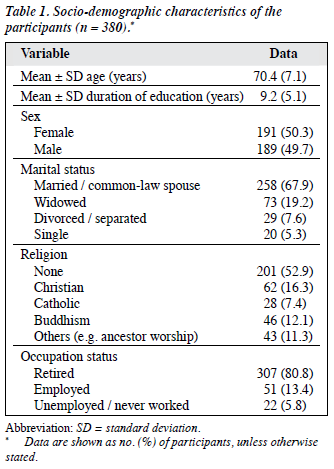
A total of 380 participants (189 men and 191 women) took part in the study. The mean ± standard deviation (SD) age was 70.4 ± 7.1 years (range, 60-97 years), with a mean duration of education of 9.2 ± 5.1 years (range, 0-24 years). In all, 306 participants (81%) had a CDR score of 0 and a mean CMMSE score of 28.8 ± 1.3 (range, 24-30). Also, 74 (20%) participants had a CDR score of 0.5 and a mean CMMSE score of 25.4 ± 2.2 (range, 21-30). The socio- demographic data of the participants are shown in Table 1.
Leisure Activities
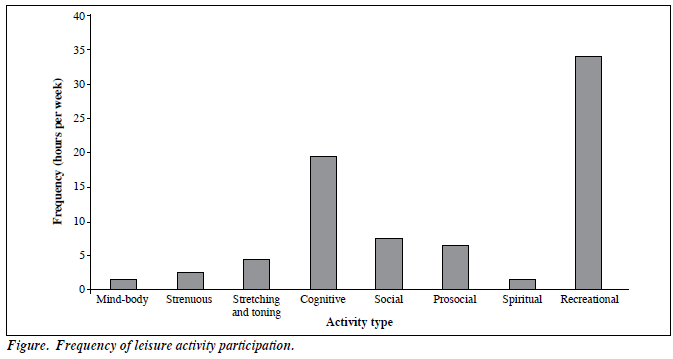
In all, 99.7% of the participants reported recreational activity, cognitive activity, and social activity as the most common leisure activities that they had engaged in during the previous year. About half of the participants engaged in prosocial activity and spiritual activity. Stretching and toning exercises (73.4%) were the most common physical activities engaged in by the participants, followed by aerobic exercise (46.6%) and mind-body exercise (27.6%). The Figure shows the frequency of leisure activity participation in each domain.
Association with Cognitive Function
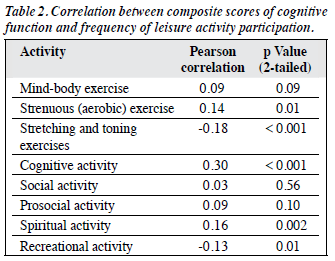
The composite score for cognitive function was negatively correlated with stretching and toning exercises and positively correlated with aerobic exercise, cognitive activity, and spiritual activity. Participants with poor cognitive function preferred stretching and toning exercises to other types of exercise. Table 2 shows the correlation between cognitive function and frequency of activity participation.
Linear regression analysis was conducted to determine whether the composite cognitive score was closely associated with the frequency of activity. After controlling for age and years of education, nearly half the variation (R2 = 52.1%) in the composite cognitive score could be explained by the frequency of cognitive activity (B = 0.87, beta = 0.22; 95% confidence interval [CI] = 0.52- 1.25 and p < 0.001) and spiritual activity (B = 0.45, beta = 0.11; 95% CI = 0.13-0.76 and p = 0.01).
Association with Purpose in Life
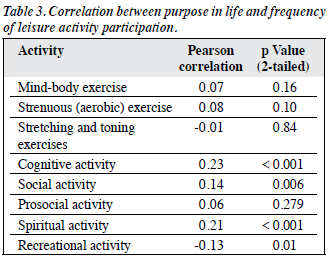
The score for purpose in life was positively correlated with spiritual activity, cognitive activity, and social activity (Table 3). Linear regression was conducted to determine whether purpose in life could be predicted from the frequency of activity participation. The results showed that spiritual activity (B = 5.30, beta = 0.18; 95% CI = 2.45-8.15 and p ≤ 0.0001), social activity (B = 4.93, beta = 0.18; 95% CI = 2.13-7.73 and p = 0.001), and cognitive activity (B = 4.57, beta = 0.16; 95% CI = 1.31-7.82 and p = 0.01) were associated with a higher score for purpose in life. When the results were then further controlled for loneliness in addition to age and years of education, only spiritual activity (B = 4.68, beta = 0.16; 95% CI = 2.21-7.14 and p ≤ 0.001) was able to predict a higher score for purpose in life.
Linear regression was also conducted to determine whether cognitive function could be predicted from purpose in life. The results suggested that better cognitive function was associated with a higher score of purpose in life independent of age and years of education (B = 1.99, beta = 0.28; 95% CI = 1.10-2.87 and p < 0.001). The interaction between frequency of spiritual activity and purpose in life score and the effect on cognitive function was also examined. The main effects of spiritual activity (B = 0.42, beta = 0.10; 95% CI = 0.09-0.75 and p = 0.01) and purpose in life (B = 5.709, beta = 0.18; 95% CI = 3.22-8.19 and p < 0.001) were significant. The effect on cognitive function was also significant (B = 0.23, beta = 0.12; 95% CI = 0.70- 0.38 and p = 0.01).
Discussion
These findings suggest that late-life cognitive and spiritual activities are associated with better cognitive function. While the effect of late-life cognitively stimulating activity has been well studied, the effect of spiritual activity on cognition has not been comprehensively studied.
We adapted and modified the activity questionnaire initially designed to measure leisure activity profiles in older Chinese adults.33 After revision of the original activity classification, we believed that reciprocal behaviour and spiritual activity are different from some of the more commonly defined social activities such as singing and social gathering with friends. Spiritual activity may play a role in fostering hope when encountering adversity, which may enhance positive affect and improve endurance of negative life events such that self-actualisation may be achieved. The new 6-domain classification may enable us to examine different leisure activities more comprehensively.
Spiritual activity includes engaging in regular religious rituals and meditation. Extensive findings have demonstrated that spirituality is correlated with a variety of positive mental health outcomes, including lower rate of depression, higher self-esteem, and better quality of life.40-42 Emerging data also suggest that active involvement in spiritual activity is associated with slow progression of AD. Coin et al40 examined the relationship between religiosity and the development of cognitive impairment in people living with AD. The low-religiosity group experienced significantly greater decline in cognitive performance after 12 months than did the high-religiosity group. Kaufman et al41 also assessed the effect of spirituality and religiosity on people with probable AD. This longitudinal study found that older adults with higher levels of spirituality and religiosity declined less rapidly. Spiritual activity may be qualitatively different from cognitively stimulating activity as it was found to be associated with subjective well-being.43 Future studies could focus more on how spiritual activity may act as a modulating factor that contributes to protection against dementia through improving other positive mental health outcomes.
Although the relationship among spiritual activity, psychological well-being, and cognitive function could not be inferred directly, our results suggest that spiritual activity is associated with purpose in life. Previous cross-sectional studies have found that purpose in life is associated with psychological well-being such as happiness, satisfaction with life, personal growth, self-acceptance, and better sleep.44-47 A 7-year prospective study by Boyle et al25 found that older adults with a greater purpose in life were more likely to maintain cognition than those with a low purpose in life. Our findings suggest that there is an interaction between spiritual activity and purpose in life resulting in better cognition. These results suggest that cognitive function may be modulated by spiritual activity and purpose in life through a pathway that connects spiritual activity and purpose in life.
It would be of interest to study the association between spiritual activity and brain function. Functional imaging study has demonstrated that the repetitive practice of meditation in daily life enhances brain connectivity48 and increases prefrontal cortical thickness49 and grey matter density in the lower brain stem region.50 These results might account for the effect of enhancing attention and maintaining cognition in old age.
In this study, we used a self-report method to obtain information on activity participation among elderly people. This method has limitations in terms of reliability and validity. One of the challenges in obtaining the frequency of activity participation is that elderly people do not necessarily maintain consistent behaviour for certain activities. Therefore, it may be helpful to ascertain a time frame when asking about the frequency of activities performed.
Conclusion
Out findings suggest that a higher level of spiritual activity and a high purpose in life in later life are both associated with better cognitive function. Longitudinal studies are recommended to further examine the causal relationship of spiritual activity and cognitive function in older adults.
Declaration
The authors declared no actual or potential conflict of interest in relation to this article.
References
- United Nations, Department of Economic and Social Affairs, Population Division. World population prospects: the 2010 revision, CD-ROM edition. New York: United Nations; 2011. Available from: http://www.un.org/en/development/desa/publications/world-population-prospects-the-2010-revision.html. Accessed 19 August 2013.
- Fung AW, Leung GT, Lam LC. Modulating factors that preserve cognitive function in healthy ageing. East Asian Arch Psychiatry 2011;21:152-6.
- Ganguli M, Vander Bilt J, Saxton JA, Shen C, Dodge HH. Alcohol consumption and cognitive function in late life: a longitudinal community study. Neurology 2005;65:1210-7.
- Lam LC, Tam CW, Lui VW, Chan WC, Chan SS, Chiu HF, et al. Modality of physical exercise and cognitive function in Hong Kong older Chinese community. Int J Geriatr Psychiatry 2009;24:48-53.
- Oken BS, Zajdel D, Kishiyama S, Flegal K, Dehen C, Haas M, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med 2006;12:40-7.
- Leung GT, Fung AW, Tam CW, Lui VW, Chiu HF, Chan WM, et al. Examining the association between late-life leisure activity participation and global cognitive decline in community-dwelling elderly Chinese in Hong Kong. Int J Geriatr Psychiatry 2011;26:39-47.
- Cheng ST, Chan AC, Yu EC. An exploratory study of the effect of mahjong on the cognitive functioning of persons with dementia. Int J Geriatr Psychiatry 2006;21:611-7.
- Wilson RA, Mendes De Leon CF, Barnes LL, Schneider JA, Bienias JL, Evans DA, et al. Participation in cognitively stimulating activities and risk of incident Alzheimer disease. JAMA 2002;287:742-8.
- Hall CB, Lipton RB, Sliwinski M. Cognitive activities delay onset of memory decline in persons who develop dementia. Neurology 2009;73:356-61.
- Verghese J, LeValley A, Derby C, Kuslansky G, Katz M, Hall C, et al. Leisure activities and the risk of amnestic mild cognitive impairment in the elderly. Neurology 2006;66:821-7.
- Verghese J, Lipton RB, Katz MJ, Hall CB, Derby CA, Kuslansky G, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med 2003;348:2508-16.
- Pillai JA, Hall CB, Dickson DW, Buschke H, Lipton RB, Verghese J. Association of crossword puzzle participation with memory decline in persons who develop dementia. J Int Neuropsychol Soc 2011;17:1006- 13.
- Dik M, Deeg DJ, Visser M, Jonker C. Early life physical activity and cognition at old age. J Clin Exp Neuropsychol 2003;25:643-53.
- Van Gelder BM, Tijhuis MA, Kalmijn S, Giampaoli S, Nissinen A, Kromhout D. Physical activity in relation to cognitive decline in elderly men: the FINE study. Neurology 2004;63:2316-21.
- Larson EB, Wang L, Bowen JD, McCormick WC, Teri L, Crane P, et al. Exercise is associated with reduced risk for incident dementia among persons 65 years of age and older. Ann Int Med 2006;144:73- 81.
- Lam LC, Chau RC, Wong BM, Fung AW, Tam CW, Leung GT, et al. A 1-year randomized controlled trial comparing mind body exercise (Tai Chi) with stretching and toning exercise on cognitive function in older Chinese adults at risk of cognitive decline. J Am Med Dir Assoc 2012;13:568.e15-20.
- Lautenschlager NT, Cox KL, Flicker L, Foster JK, van Bockxmeer FM, Xiao J, et al. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease: a randomized trial. JAMA 2008;300:1027-37.
- Snowdon DA. Aging and Alzheimer’s disease: lessons from the Nun Study. Gerontologist 1997;37:150-6.
- Reyes-Ortiz CA, Berges IM, Raji MA, Koenig HG, Kuo YF, Markides KS. Church attendance mediates the association between depressive symptoms and cognitive functioning among older Mexican Americans. J Gerontol A Biol Sci Med Sci 2008;63:480-6.
- Corsentino EA, Collins N, Sachs-Ericsson N, Blazer DG. Religious attendance reduces cognitive decline among older women with high levels of depressive symptoms. J Gerontol A Biol Sci Med Sci 2009;64:1283-9.
- Prakash R, Rastogi P, Dubey I, Abhishek P, Chaudhury S, Small BJ. Long-term concentrative meditation and cognitive performance among older adults. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn 2012;19:479-94.
- Bolt M. Purpose in life and religious orientation. J Psychol Theol 1975;3:116-8.
- Donahue MJ. Intrinsic and extrinsic religiousness: review and meta- analysis. J Pers Soc Psychol 1985;48:400-19.
- Tomer A, Eliason G. Beliefs about self, life, and death: testing aspects of a comprehensive model of death anxiety and death attitudes. In: Tomer A, editor. Death attitudes and the older adult: theories, concepts, and applications. Philadelphia, PA: Brunner-Routledge; 2000: 137-53.
- Boyle PA, Buchman AS, Barnes LL, Bennett DA. Effect of a purpose in life on risk of incident Alzheimer disease and mild cognitive impairment in community-dwelling older persons. Arch Gen Psychiatry 2010;67:304-10.
- Myers DG. The funds, friends, and faith of happy people. Am Psychol 2000;55:56-67.
- Swinyard WR, Kau AK, Phua HY. Happiness, materialism, and religious experience in the US and Singapore. J Happiness Stud 2001;2:13-32.
- Krause N. Religious meaning and subjective well-being in late life. J Gerontol B Psychol Sci Soc Sci 2003;58:S160-70.
- Morris JC. Clinical dementia rating: a reliable and valid diagnostic and staging measure for dementia of the Alzheimer type. Int Psychogeriatr 1997;9 Suppl 1:173-6.
- Chiu HF, Lee HC, Chung WS, Kwong PK. Reliability and validity of the Cantonese version of the Mini-Mental State Examination: preliminary study. J Hong Kong Coll Psychiatrists 1994;4:25-8.
- Mok EH, Lam LC, Chiu HF. Category verbal fluency test performance in Chinese elderly with Alzheimer’s disease. Dement Geriatr Cogn Disord 2004;18:120-4.
- de Zubicaray GI, Smith GA, Chalk JB, Semple J. The Modified Card Sorting Test: test-retest stability and relationships with demographic variables in a healthy older adult sample. Br J Clin Psychol 1998;37:457-66.
- Leung GT, Leung KF, Lam LC. Classification of late-life leisure activities among elderly Chinese in Hong Kong. East Asian Arch Psychiatry 2011;21:123-7.
- Crumbaugh JC, Maholick LT. An experimental study in existentialism: the psychometric approach to Frankl’s concept of noogenic neurosis. J Clin Psychol 1964;20:200-7.
- Shek DT. Meaning in life and psychological well-being: an empirical study using the Chinese version of the purpose in life questionnaire. J Genet Psychol 1992;153:185-200.
- Seeman M. Alienation and anomie. In: Robinson JP, Shaver PR, Wrightsman LS, editors. Measures of personality and social psychological attitudes, Volume I. San Diego, CA: Academic Press; 1991: 291-371.
- Parmelee PA, Thuras PD, Katz IR, Lawton MP. Validation of the Cumulative Illness Rating Scale in a geriatric residential population. J Am Geriatr Soc 1995;43:130-7.
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders. Clinical descriptions and diagnostic guidelines. Geneva: WHO; 1992.
- Brugha TS, Bebbington PE, Jenkins R, Meltzer H, Taub NA, Janas M, et al. Cross validation of a general population survey diagnostic interview: a comparison of CIS-R with SCAN ICD-10 diagnostic categories. Psychol Med 1999;29:1029-42.
- Coin A, Perissinotto E, Najjar M, Girardi A, Inelmen EM, Enzi G, et al. Does religiosity protect against cognitive and behavioral decline in Alzheimer’s dementia? Curr Alzheimer Res 2010;7:445-52.
- Kaufman Y, Anaki D, Binns M, Freedman M. Cognitive decline in Alzheimer disease: impact of spirituality, religiosity, and QOL. Neurology 2007;68:1509-14.
- Maselko J, Gilman SE, Buka S. Religious service attendance and spiritual well-being are differentially associated with risk of major depression. Psychol Med 2009;39:1009-17.
- Ellison CG. Religious involvement and subjective well-being. J Health Soc Behav 1991;32:80-99.
- Ryff CD, Singer BH, Dienberg Love G. Positive health: connecting well-being with biology. Philos Trans R Soc Lond B Biol Sci 2004;359:1383-94.
- Ryff CD, Keyes CL. The structure of psychological well-being revisited. J Pers Soc Psychol 1995;69:719-27.
- Wrosch C, Scheier MF, Miller GE, Schulz R, Carver CS. Adaptive self-regulation of unattainable goals: goal disengagement, goal reengagement, and subjective well-being. Pers Soc Psychol Bull 2003;29:1494-508.
- Boyle PA, Barnes LL, Buchman AS, Bennett DA. Purpose in life is associated with mortality among community-dwelling older persons. Psychosom Med 2009;71:574-9.
- Luders E, Clark K, Narr KL, Toga AW. Enhanced brain connectivity in long-term meditation practitioners. Neuroimage 2011;57:1308-16.
- Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thickness. Neuroreport 2005;16:1893-7.
- Vestergaard-Poulsen P, van Beek M, Skewes J, Bjarkam CR, Stubberup M, Bertelsen J, et al. Long-term meditation is associated with increased gray matter density in the brain stem. Neuroreport 2009;20:170-4.