East Asian Arch Psychiatry 2014;24:3-9
ORIGINAL ARTICLE
吴倩华、卢惠如、梁启新、陈秀敏、黄天欣、林伟德、曾洁莹
Dr Serena S. W. Ng, EdD, MSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Ms Ada W. Y. Lo, MSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Mr Tony K. S. Leung, MSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Ms Frances S. M. Chan, MSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Ms Asta T. Y. Wong, MSocSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Mr Ronny W. T. Lam, MMedSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Ms Delia K. Y. Tsang, MSc, Occupational Therapy Department, Kowloon Hospital, Hong Kong SAR, China.
Address for correspondence:
Tel: (852) 3129 6070 ; Fax: (852) 2624 7401; email: ngsws@ha.org.hk
Submitted: 13 June 2013; Accepted: 15 August 2013
Abstract
Objective: Quality of life outcomes are useful in the assessment of mental and social wellbeing and for informed health care decision-making, especially in the choice of interventions in psychiatric rehabilitation. In its original form, the Warwick-Edinburgh Mental Well-being Scale (WEMWBS) is a proven reliable and valid tool for assessing quality of life in normal adults, but not in adults from Asian countries. A shortened 7-item version of WEMWBS (SWEMWBS) with good internal construct validity was used for this study. The present study describes the translation of WEMWBS from English to Chinese and its validation in a sample of Chinese-speaking patient population.
Methods: Participants included patients admitted to the inpatient units, and those attending the day hospital and outpatient units of the Kowloon Hospital (n = 126). Translation was performed using the multiple forward and backward translation protocol. Patients also completed the 5-item World Health Organization Well-being Index (WHO5) questionnaire. A case therapist completed the Brief Psychiatric Rating Scale within 2 days. A total of 20 patients were selected for test-retest measurements performed after 2 weeks.
Results: The sample displayed a normal distribution of the Chinese version of SWEMWBS (C-SWEMWBS) scores (mean ± standard deviation, 23.16 ± 5.39; skewness, -0.068; kurtosis, -0.355). Internal reliability coefficient (Cronbach’s alpha) for C-SWEMWBS was 0.89 which was consistent with that of English version. The corrected item-total correlation was high with Spearman’s rank correlation coefficients ranging from 0.57 (item 6) to 0.75 (item 5). Good test- retest reliability was observed (r = 0.677; p = 0.001). Principal components factor analysis identified a single component (eigenvalues, 4.28; 61.1% variance), similar to the English version. Scores of C- SWEMWBS were positively correlated with the scores of WHO5 (r = 0.49; p < 0.001), suggesting good concurrent validity. Few item scores including ‘feeling useful’, ‘dealing with problems well’, ‘able to make decisions’, and the total score were significantly correlated with diagnostic groups (p < 0.05). Education and diagnosis of mental illness were valid predictors for C-SWEMWBS (F = 5.41; p = 0.01). There were no effects due to age and gender.
Conclusion: The C-SWEMWBS showed high levels of internal consistency and reliability against accepted criteria. It is short, acceptable, and culturally meaningful to clients with mental illness. Further large-scale studies in normal subjects and varied patient groups are recommended to generalise the findings.
Key words: Mental disorders; Mental health; Quality of life
摘要
目的:生活质素的结果对评估精神和社会健康,以及对医疗方案的决定,尤於精神复康的干预选择方面有实际意义。沃里克爱丁堡心理健康量表(WEMWBS)能可靠并準确评估一般成人的生活质素,但这并不包括亚洲人口。因此,本研究使用具有良好内部结构效度的简短7项版本(SWEMWBS),并检视其英译中版本於汉语患者人口的效度。
方法:参与者包括香港九龙医院入院患者,以及日诊和门诊患者(n = 126)。量表采用多重顺向及逆向翻译方法。患者并完成世界卫生组织五项身心健康指标(WHO5)问卷,而治疗师则於患者完成问卷後2天内完成简易精神病评定量表。共20名患者被挑选於2週後再完成相关问卷 以评估其重测信度。
结 果 : S W E M W B S 中 文 版 ( C - S W E M W B S ) 的 分 数 呈 正 态 分 佈 ( 平 均 ± 标 準 差,23.16 ± 5.39;偏度-0.068;峰度-0.355);其内部信度係数(Cronbach's alpha)则为0.89,与英语版本一致。修正後项目总分相关係数高,Spearman等级相关係数介乎0.57(第6 项)至0.75(第5项)。C-SWEMWBS也具良好的重测信度(r = 0.677;p = 0.001)。主成分 分析确定了单一成分(特徵值4.28;具61.1%的变异),这也与英文版本相若。C-SWEMWBS 得分与WHO5得分也呈正相关(r = 0.49;p < 0.001),这表明良好的同时效度。此外,部份 项目得分如「自觉有用」、「能解决问题」、「能作决策」,以及总比分与诊断组呈显著相关(p < 0.05)。教育与诊断是C-SWEMWBS的有效预测因子(F = 5.41;p = 0.01)。年龄和性 别对C-SWEMWBS得分并没有影响。
结 论 : 相 对 其 他 可 接 受 的 标 準 , C - S W E M W B S 表 现 出 高 水 平 的 内 部 一 致 性 和 可 靠 性 。 C - SWEMWBS是对精神病患者既简短、可接受且具文化意义的评估工具。可考虑进一步於一般人 口和不同患者群组中进行大规模研究,使研究结果更能概括化。
关键词:精神障碍、精神健康、生活质素
Introduction
Quality of life (QOL) is a subjective experience and QOL measurements must rely on the clients’ self reports. Quality- of-life outcomes are useful in the assessment of mental and social wellbeing and for informed health care decision- making, especially in the choice of interventions. Tools such as the 28-item World Health Organization Quality of Life brief questionnaire and 36-item Short-Form Health Survey are commonly used for evaluating QOL in psychiatric rehabilitation. But these are either too broad in scope or focused only on health-related impacts. Besides, local clinicians may find these tools too lengthy and inconvenient for use in daily clinical practice. Currently, there is lack of a reliable instrument that can systematically evaluate the QOL based on views about well being expressed by patients with mental illnesses. As members of the mental health workforce, occupational therapists emphasise on reconstructing meaningful life for their clients suffering from various mental conditions such as schizophrenia, bipolar disorder, mood disorders, and adjustment disorders. They use several instruments to assess dysfunction and daily living problems, but lack a brief but reliable tool for evaluating the impact of interventions on their patients’ wellbeing.
It is now popular for nations to develop assessment tools to measure the wellbeing of the population. Data show that mental wellbeing contributes to all aspects of human life, and has significant health and social consequences.1-3 The Warwick-Edinburgh Mental Well-being Scale (WEMWBS) is one of this newly developed scales for assessing an individual’s mental health (mental wellbeing). It comprises 14 positively worded items, with 5 response categories. It covers most aspects of positive mental health (positive thoughts and feelings) currently described in the literature, including both hedonic and eudaimonic perspectives.4 In its original form, the WEMWBS is a proven, reliable and valid tool for assessing QOL in normal adults, However, its validity and reliability have not been proven in adults from Asian countries, or in patient populations. Thus, we undertook the exercise to translate and introduce the first validated Chinese version of the SWEMWBS (C- SWEMWBS). A shortened 7-item version (SWEMWBS)5 with good internal construct validity was used for this study in view of its ease of administration to the target population and brevity, given the time constraints in clinical settings.
The SWEMWBS is an ordinal scale comprising 7 positively phrased Likert-style items. Items covered a range of aspects of mental wellbeing including those from other well-known scales. Responses in the form of a Likert scale included ‘none of the time’ (scored 1), ‘rarely’ (2), ‘some of the time’ (3), ‘often’ (4), and ‘all of the time’ (5). Scores ranged from 7 to 35, with a high score reflecting a high level of mental wellbeing. The scale was validated with students and representative population samples from UK using qualitative as well as quantitative methods, and performed well against criteria for scale development.5 It showed good content validity, moderately high correlations with other mental health scales and lower correlations with other scales measuring overall health. Its distribution was near normal and did not show ceiling effects in population samples. It discriminated between population groups in a way that is largely consistent with the results of other population surveys.5
The present study describes the translation of SWEMWBS from English to Chinese and its validation in Chinese-speaking patients. This is the first Chinese version of SWEMWBS and also the first time it has been validated in patients with mental illness.
Methods
Participants
The participants in this study were patients admitted to the inpatient psychiatric observation unit, and attending the day hospital and outpatient units of Kowloon Hospital in Hong Kong. Only those participants who could read and write traditional Chinese with no significant or diagnosed cognitive problems and were mentally stable for giving informed consent were included in the study. The research proposal was approved by the Research Ethics Committee of Kowloon Central / East Cluster, Hospital Authority of Hong Kong. All subjects were invited to participate voluntarily in the study. Eligible candidates were required to complete the translated version of the SWEMWBS questionnaire. They had the right to withdraw from the study without giving any reasons.
Instruments
The C-SWEMWBS was cross-culturally adapted from the original English version (available with permission from the developers) using standard guidelines, including independent forward and backward translations and reviewed by an expert panel. In this study, we used the self- report version of SWEMWBS.4
The Brief Psychiatric Rating Scale6 (BPRS) is used to measure psychiatric symptoms such as depression, anxiety, hallucinations, and unusual behaviour. Each symptom is rated from 1 to 7, and a total of 24 symptoms are scored with the highest possible score of 168.7
The 5-item World Health Organization Well-being Index8 (WHO5) is an internationally validated 5-item easy- to-use tool that reflects the general wellbeing status in the recent 2 weeks. The score of each item ranges from 0 (‘at no time’) to 5 (‘all of the time’), therefore the possible total score is in the range of 0 to 25. A total score of < 13, or any item scored ≤ 1 indicate poor wellbeing and mood problems. This scale was adopted in this study as a concurrent validation tool in the same area of testing.
Translation Procedures
The translation strategy was based on minimal criteria developed by the Scientific Advisory Committee of the Medical Outcomes Trust (1997). Translation was performed using the multiple forward and backward translation protocol.9 Following these, 3 independent bilingual health care professionals translated the questionnaire into Chinese (forward translation). The mother tongue of all translators was Chinese language and they had a high level of the English language. A reconciliation meeting through emails was conducted to obtain a consensus version. Then, 2 native English teachers (one teaching at a secondary school and the other at a university) who were blinded to the original version retranslated the Chinese version to the source language (back-translation). The back-translation was sent to the developer; her suggestions were taken into account and after amendment, the final version was re-sent for endorsement. This was the process of formulation of the final C-SWEMWBS.
Pretesting of the translated scale was done in a small sample of 5 occupational therapists who had at least 3 years of experience in mental health services, and 5 patients who did not have any previous experience with the instrument. In-depth understanding of the questions with the purpose of reviewing inappropriate words was emphasised to ensure semantic and content equivalence. Content of the review included clarity of the items, relevance of the content to their situations, the neatness of instructions, and ability to complete the test on their own. The 5 occupational therapists and 5 patients were asked to make suggestions wherever necessary. No revision was proposed after this focus review. Results were sent to the developer for endorsement of the final version. The time required for completion of this process was 2 months (Fig).
Data Collection

Convenience sampling was used for recruiting 126 patients from the inpatient (n = 60), outpatient (n = 34), and day hospital (n = 32) units. They were interviewed by case therapists to complete the informed consent and database forms. They were then given 2 assessment forms for self- completion, namely, the C-SWEMWBS and WHO5. Case therapists also completed the BPRS within 2 days for patients who successfully completed the scales. A total of 20 patients were selected from this sample to complete the 2 self-report assessment forms 2 weeks later for test-retest measurements.
Data Analysis
The normality of the items of all measures was investigated and an acceptable range of skewness of < 2 and kurtosis of < 7 was adopted.10 Principal components factor analysis was utilised to assess the internal structure of the measure. Internal consistency and reliability were assessed using Cronbach’s alpha coefficient and item correlations. Alpha coefficients of ≥ 0.70 and item-total correlation of > 0.4 were used to indicate good reliability.11,12 Concurrent validity was assessed by using the Spearman’s rank correlation to examine the relationship between C-SWEMWBS and WHO5. A p value of < 0.05 was considered to denote a statistically significant finding. All statistical analyses were performed using SPSS version 19.0.
Results
Demographics
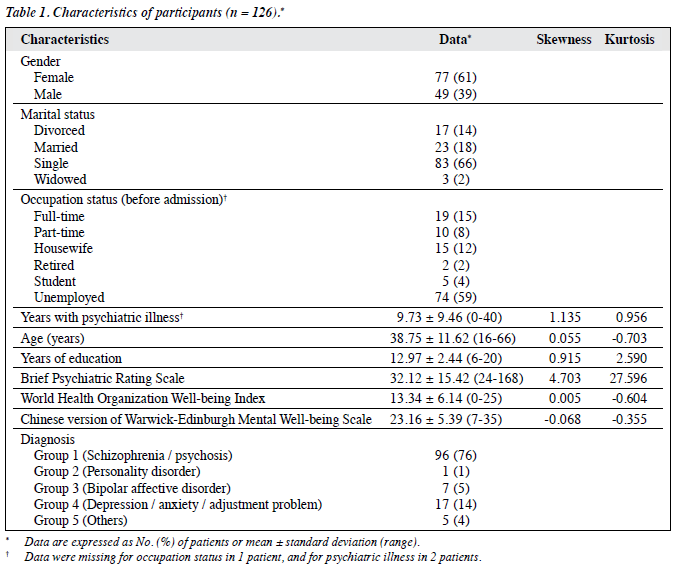
Demographics of the participants are shown in Table 1. Of these 126 participants, 77 were female and 49 were male. Their mean ± standard deviation (SD) age was 38.75 ± 11.62 (range, 16-66) years. In all, 94 participants (75%) had received up to secondary level of education and 29 (23%) up to the tertiary level. Overall, 23 participants (18%) were married and 83 (66%) were single; the remaining 20 participants were either divorced or had lost their spouse. Prior to admission, 74 participants (59%) were unemployed, 15% and 8% were working full-time or part-time, respectively, and the remaining were housewives (12%) and students (4%). Their mean duration of psychiatric illness was 9.73 ± 9.46 years (range, 0-40 years).
Profile of Psychiatric Symptoms
All 126 participants were divided into 5 diagnostic groups. Overall, 96 (76%) had schizophrenia or psychosis, 1 (1%) had personality disorder, 7 (5%) had bipolar affective disorder, 17 (14%) had adjustment problem, depression or anxiety, and the others (4%) had anorexia (n = 1), substance abuse (n = 3), and autism (n = 1). The BPRS total score ranged from 24 to 168, with a mean of 32.12 ± 15.42 (skewness, 4.703; standard error, 0.22). In individual item rating, 13 (10%) cases had BPRS score of ≥ 5 in 1 or more symptoms; 48 (38%) cases scored 3 or 4 in at least 1 symptom; and the remaining 65 cases (52%) were assessed to have very mild symptoms. The most commonly reported symptoms included anxiety, disorientation, unusual thought content, grandiosity, depression, suspiciousness, guilt, hostility, and elated mood. Twelve of them (10%) showed moderately severe to extremely severe symptoms in terms of anxiety, guilt, suspiciousness, unusual thought content, disorientation, and conceptual disorganisation; 65 cases (52%) displayed only mild-to-moderate depression and anxiety symptoms. Overall, 48 cases (38%) suffered from a spectrum of symptoms which ranged from mild to moderate level in severity. Thus, the sample was not homogeneous in terms of presentation and severity of psychiatric symptoms.
Subjective Wellbeing Status
The mean WHO5 score of the sample was normally distributed (13.34 ± 6.14; skewness, 0.005). This indicated a borderline wellbeing problem in our sample. Of the 126 subjects, 54 (43%) reported poor wellbeing status (mean score, 7.56 ± 3.27) and the remaining 72 (57%) reported comparatively better scores (17.68 ± 3.73). The lowest scores were noted in items related to vitality (‘having energy’ and ‘waking up fresh and rested’), while the highest scores were noted in items related to positive mood (‘feeling relaxed’). The mean score for those with schizophrenia was 12.78 ± 5.99 and for those with personality disorder it was 8.00 ± 3.44; both were below the cut-off score of 13. However, the mean total scores of participants across these 5 diagnostic groups were not significantly different.
The mean C-SWEMWBS score of the sample was 23.16 ± 5.39 (range, 7-35). The highest score was observed in patients suffering from autism, anorexia, and substance abuse (mean score, 27.2 ± 4.7) while the lowest score was reported by the subject with personality disorder (mean score, 17.0). Similar to the results in WHO5 index, there was no significant difference between the mean scores of these 5 diagnostic groups, probably due to uneven distribution of the sample and small sample size of each group.
Scale Reliability
Internal Consistency
The sample displayed a normal distribution of C- SWEMWBS scores (mean ± SD, 23.16 ± 5.39; skewness, -0.068; kurtosis, -0.355). Internal reliability coefficient for C-SWEMWBS was 0.89. This finding is consistent with that of the English version (0.89, student sample) and just lower than 0.91 of the population sample.13 The corrected item-total correlation was high, with Spearman’s rank correlation coefficients ranging from 0.57 (item 6) to 0.75 (item 5) [Table 2].
Test-retest Reliability
Of the 126 participants, 20 were randomly selected with convenient subsampling to evaluate the test-retest reliability in 2 weeks’ time. Cronbach’s alpha for this subset in the initial test period was 0.84 (95% confidence interval, 0.71- 0.93; p < 0.001) and 0.92 (0.87-0.97; p < 0.001) in the retest period. Correlation between the test and retest mean scores of these participants was likewise high (r = 0.677; p = 0.001), suggesting a high reliability for the Chinese version of the scale in test-retest.
Construct Validity
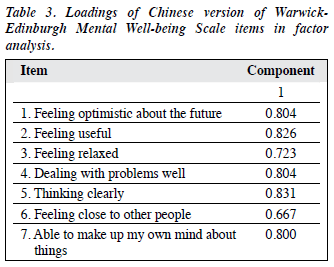
Factor loadings were analysed by principal components factor analysis with varimax rotation. The analysis identified a single component (eigenvalues, 4.28; 61.1% variance)

which confirmed that the Chinese version measured the same construct as the English version (Table 3).
Concurrent Validity
Scores of C-SWEMWBS were found to correlate positively with the scores of WHO5 (r = 0.49; p < 0.001), suggesting a moderate association between subjective wellbeing and mental wellbeing. Hence, the C-SWEMWBS may cover other areas of wellbeing items perceived by the clients as different from WHO5 index. In fact, the correlation between WHO5 score and BPRS score was high (r = –0.231; p = 0.01), which might indicate the direct effects of illness symptoms on the assessed areas such as sleep quality, mood fluctuations, etc. However, there was no significant correlation between BPRS and C-SWEMWBS score, although the latter shares few items similar in its content with WHO5 index. Thus, C-SWEMWBS might reflect a more comprehensive wellbeing status than WHO5 in terms of the perception of wellbeing by an individual as a stable and long-term factor.
Age, Education, and Gender Effect
Spearman’s rank correlation revealed that C-SWEMWBS total score was not correlated with age, gender, years of psychiatric illness, and pattern of psychiatric symptoms (BPRS). However, it showed moderate correlation with years of education (r = 0.223; p = 0.01).
Application in Psychiatry
Partial correlation was performed using diagnostic groups and scorings of C-SWEMWBS, with years of education controlled. There were significant correlations in the scores of items ‘feeling useful’ (r = 0.194; p = 0.03), ‘dealing with problems well’ (r = 0.197; p = 0.03), ‘able to make decisions’ (r = 0.18; p = 0.05), and the total score (r = 0.186; p = 0.04). Stepwise linear regression showed that education and diagnosis of mental illness were predictors of high C-SWEMWBS total score (R2 = 0.082; F = 5.41; p = 0.01). However, no significant difference was noted in the mean C-SWEMWBS scores among the different diagnostic groups, probably due to the small sample size.
Discussion
The present study sought to provide a reliable and valid measure of mental wellbeing for use among Chinese- speaking patients with mental illness in Hong Kong. Results showed that the translated version of C-SWEMWBS was a reliable and valid measure in our study sample. A relatively short 7-item questionnaire C-SWEMWBS showed good internal consistency (Cronbach’s alpha, 0.89). and stability over a period of 2 weeks among the selected clients, although the sample size was small. Moreover, the scale showed significant correlations with WHO5 (r = 0.49; p < 0.001) suggesting good concurrent validity. The results of this study also showed high validity of the scale. Principal components factor analysis supported a single concept of measurement, i.e. positive mental attributes, which was not significantly correlated with any specific mental illness or patterns of mental symptoms under BPRS.
The scoring of C-SWEMWBS appears to be less prone to bias than the other wellbeing scales used in this study as there was only moderate correlation with years of education and no correlation with age or gender. Nevertheless, there was correlation of C-SWEMWBS with different psychiatric diagnoses, although no significant difference in the mean scores was obtained across the different diagnostic groups. This suggests areas for further research for mental health workers. These may include fields of problem-solving, choice and decision-making, and feeling of being useful, which may serve to improve the patients’ wellbeing despite having symptoms of illness. Availability of C-SWEMWBS will be a huge advantage as it will now be possible to reliably measure mental wellbeing among Chinese patients with mental illness. It also poses opportunities for more research for developing and evaluating interventions aimed at improving wellbeing of individuals.
Limitations
This study has a number of limitations. The sample was collected from a single local hospital; further studies in large samples from diverse populations are needed for generalisation of the results to the whole psychiatric population. The sequence of testing was not randomised and may confound results with order effects. The small number of sample in test-retest, owing to operational problems, may pose errors in analysis. Besides, whether the stability of the measure can be extended to more than 2 weeks also needs further investigation. In addition, the scale’s capacity to detect changes in mental wellbeing at both individual and population levels has not been explored in this study. Although the properties of C-SWEMWBS are similar to that of the WHO5, it may help to discriminate problematic wellbeing status. Further studies are needed to improve the application of the scale in other areas, e.g. a norm study across populations with different psychiatric illnesses or in normal populations.
Conclusion
The C-SWEMWBS shows high level of internal consistency and reliability against accepted criteria. It is short, acceptable, and culturally meaningful to the Chinese patients with mental illness in various stages of treatment. Further validity and reliability studies in a larger sample size are needed to ascertain the generalisation of findings. Furthermore, its potential to detect differences of wellbeing status across patients with various diagnoses or normal people needs to be further explored through local studies for developing normative data and sensitivity of changes.
References
- Herrman H, Moodie R, Saxena S. Promoting mental health: concepts, emerging evidence, practice: summary report. Geneva: World Health Organization; 2005.
- Strengthening mental health promotion. Geneva: World Health Organization; 2001.
- Ryan RM, Deci EL. On happiness and human potentials: a review of research on hedonic and eudaimonic well-being. Annu Rev Psychol 2001;52:141-66.
- Brown SS, Tennant A, Tennant R, Platt S, Parkinson J, Weich S. Internal construct validity of the Warwick-Edinburgh Mental Well- being Scale (WEMWBS): a Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual Life Outcomes 2009;7:15.
- NHS Health Scotland, The Warwick-Edinburgh Mental Well-being Scale (WEMWBS). NHS website: http://www.healthscotland.com/documents/1467.aspx. Accessed Nov 2012.
- Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep 1962;10:799-812.
- The use of psychological testing for treatment planning and outcomes. Maruish ME, editor. New Jersey: Lawrence Erlbaum Associates Inc.; 1999.
- Bech P. Measuring the dimension of psychological general well-being by the WHO-5. Quality of Life Newsletter 2004;32:15-6.
- Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 1993;46:1417-32.
- West SG, Finch JF, Curran PJ. Structural equation models with nonnormal variables. In: RH Hoyle, editor. Structural equation modeling: concepts, issues, and application. Thousand Oaks: Sage Publications; 1995: 56-75.
- 1 Clark LA, Watson D. Constructing validity: basic issues in objective scale development. Psychol Assess 1995;7:309-19.
- Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika 1951;16:297-334.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Welch S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5:63.