Hong Kong J Psychiatry 2004;14(3):15-18
ORIGINAL ARTICLE
This study was part of the UK Department for International Develop-ment (DFID)-funded longitudinal study of child poverty in 4 developing countries: Young Lives (www.younglives.org).
Dr Tran Tuan, MD, PhD, Research and Training Center for Community Development, Hanoi, Vietnam.
Dr Trudy Harpham, PhD, Professor, London South Bank University, UK.
Ms Nguyen Thu Huong, BSc, CARE International in Vietnam, Hanoi, Vietnam.
Address for correspondence: Dr Tran Tuan, Research and Training Center for Community Development-RTCCD, 39 Lane 255, Vong Street, Hanoi, Vietnam.
E-mail: directors@rtccd.org.vn
Submitted: 15 August 2003; Accepted: 7 September 2004
Abstract
Objective:The demand for inclusion of mental health measures in general health and well-being community-based surveys in developing countries is increasing. In a previous survey of child well- being in Vietnam, a measure of maternal mental health was included. This was the first use of the Self-reporting Questionnaire 20 items in Vietnam, and tested the validity and reliability. The objective of this study was to determine the sensitivity and specificity of the Self-reporting Questionnaire 20 items in Vietnam, to identify a cut-off point to determine cases, and to assess the inter-rater reliability.
Patients and Methods:Double-blind assessment was conducted for 66 rural women, half of whom had been identified as patients with mental ill health by the Self-reporting Questionnaire 20 items in a community-based survey in 2002 and half were controls. In-depth Vietnamese psychiatric appraisal and the Self-reporting Questionnaire 20 items were used for all the women. Repeat interviews were performed with the Self-reporting Questionnaire 20 items by 3 different interviewers within 24 hours.
Results:Using a cut off of 7/8, sensitivity was 73% and specificity was 82%. Inter-rater reliabil-ity combined was 0.79.
Conclusions:This study validated the first reliable, cheap, and easy-to-use, community-based measure of mental health for Vietnam.
Key words: Data collection, Reproducibility of results, Vietnam
Introduction
The demand for the inclusion of a mental health measure for general health and well-being surveys in developing countries is increasing. There have even been calls for men-tal health to be added to the influential Demographic and Health Surveys.1 To meet this demand, the World Health Organization (WHO)-recommended Self-reporting Ques-tionnaire 20 items (SRQ 20) has now been widely used and validated in many cultural contexts.2 Owing to low literacy levels in some countries, the questionnaire is usually interviewer-administered. A 4-country longitudinal study of child poverty called ‘Young Lives’ conducted in Peru, Ethiopia, India, and Vietnam included measurement of maternal mental health using the SRQ 20. No previous community-based study of mental health has been conducted in Vietnam. There was a need to test the validity and reliability of the SRQ 20 in this country, where very little is known about common mental disorders and their determinants. This paper presents the results of the tests and identifies a cut-off point to determine cases for future studies that use the SRQ 20 in Vietnam.
Patients and Methods
Instruments
The SRQ 20 has 20 yes/no questions (Table 1). The question-naire is recommended by the WHO3 and has been trans-lated into at least 20 languages.2 The English version was translated into Vietnamese and independently back-translated into English. It was then field-tested to assess appropriate use of language. The resulting Vietnamese ver-sion is available from the first author. Application by the in-terviewer takes approximately 5 minutes. The standardised in-depth psychiatric clinical interview was performed by a male Vietnamese professor of psychiatry and averaged 20 minutes.

Sampling of Respondents
As part of the longitudinal child poverty survey, the SRQ 20 had been interviewer-applied to 2000 female caregivers of 1-year-old infants across Vietnam in 2002.4 One of the 5 provinces, Hung Yen province, included in the child pov-erty survey was selected for the current study on pragmatic grounds — it was closest to Hanoi where the researchers are based. Hung Yen province, with a population of approxi-mately 1 million, is a typical rice farming, rural area with a high density — 12% of its population live below the official Vietnamese poverty line of US$209 gross domestic product per capita per annum. Forty percent of the children younger than 5 years are malnourished and the population is decreas-ing because of urbanisation.5
Six communities in Hung Yen were included in the baseline survey. Three were randomly selected for this study. Using a SRQ 20 cut-off point of 7/8 (the most commonly used cut-off point in developing countries2), the 200 female caregivers covered in the 3 communities were classified into 2 groups: women with probable mental ill health (n = 39) and controls (n = 161). The sample group for the study be-came the 39 women with probable mental ill health and 39 randomly selected women from the 161 controls (not matched). As some respondents were away from home or refused to take the tests, the final sample was 32 cases and 34 controls. Although this sample size might seem small, it is of a similar size to other validity studies and is sufficient for determining a cut-off point. All interviews were conducted in community health centres in May 2003.
Data Collection
Verbal consent was obtained from respondents by the community health centre staff 1 week prior to the inter-views. SRQ 20 interviews were conducted by 3 researchers from the Research and Training Center for Community Development, Hanoi, Vietnam. In-depth neurotic dis-order appraisal was performed by a professor of paediatric psychiatry from the General Clinic and Health Consulting Center, Hanoi, Vietnam. Female caregivers were invited by community health staff to attend the community health centre for interviews at a rate of 3 people per hour. The SRQ 20 interviews and psychiatric appraisals were conducted independently. The double-blind principle was maintained during the selection process, SRQ interviews, neurotic dis-order appraisal, and data management.
Data Analysis
In this investigation, receiver operating characteristic (ROC) analysis was used to identify a cut-off point, which maximised sensitivity and specificity.6 ROC is generally used to quantify the accuracy of a diagnostic test that is performed to discriminate between 2 states or conditions (patients and controls).
The analysis used the ROC curve — a graph of the sensitivity versus specificity of the diagnostic test. The sensitivity is the fraction of true-positive cases that were correctly identified by the SRQ 20, whereas the speci-ficity is the fraction of negative cases that were correctly classified. The performance of the test is summarised by the area under the ROC curve. This area can be interpreted as the probability that the result of a diagnostic test for a randomly selected abnormal subject will be greater than the result of the same diagnostic test for a randomly selected normal subject. The greater the area under the ROC curve, the better the performance of the test.7 ROC analysis used Stata version 8 (StataCorp, College Station, USA). Inter-rater reliability was measured using the combined statistic that was obtained from Stata version 8. Interpretation of followed the criteria of Landis and Koch.7
Ethics
Ethical approval for the larger, over-arching longitudinal child poverty study was granted by the Vietnamese Union of Scientific and Technological Associations; London South Bank University, UK; London School of Hygiene and Tropi-cal Medicine, UK; and Reading University, UK. Although the Vietnamese in-depth neurotic disorder assessor did not aim to identify causes of mental ill health, it was noted that a large number of mothers were highly anxious owing to perceptions that their child was seriously ill. To meet ethi-cal guidelines, the assessor arranged to examine the children. Of 9 children examined, 5 had no health problems. The other 4 were treated or referred.
Results
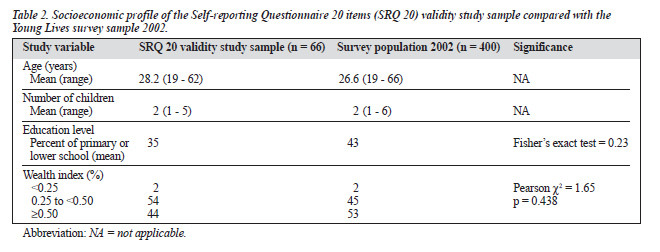
The main characteristics of the 66 women are summarised in Table 2. In comparison with the population of 400 female caregivers in the 2002 Young Lives survey of Hung Yen, there were no statistically significant differences in age, educational level, number of children, or wealth distribution.
Validation
Table 3 summarises the sensitivity and specificity of the SRQ 20 interviews from each of the 3 interviewers against the in-depth neurotic disorder appraisal. Using the SRQ 20, the probability of the correct diagnosis was maximally 79% for interviewer number 1, 82% for interviewer number 2, and 76% for interviewer number 3. The average of the 3 inter-viewers against the clinical appraisal gave a probability of correctly diagnosed cases at 79%, with a sensitivity of 73% and specificity of 82%.
The areas under the ROC curves and their 95% con-fidence intervals (CIs) are presented in Table 4. The best performance of the SRQ 20 among the 3 interviewers was noted for interviewer 2, with the area under the ROC curve at 0.86 (95% CI, 0.77-0.94). The overall performance of SRQ 20 across the 3 interviewers was high, from 0.80 to 0.86, and was not statistically significantly different. The ROC curve of the average of the 3 interviewers was 0.84 (95% CI, 0.75-0.94). No statistically significant difference was found when the 4 ROC curve areas were compared.
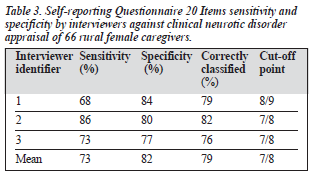
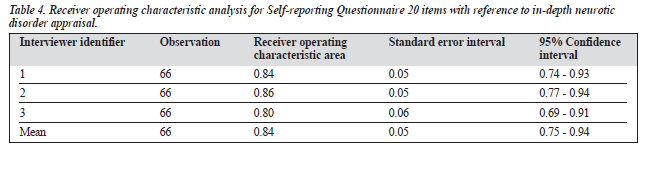
Figure 1 illustrates the average ROC curve. The cut-off point of the SRQ 20 Vietnamese version was defined at 7/8, with 73% sensitivity and 82% specificity.

Reliability
Using a cut-off point of 7/8, each female caregiver was defined as ‘not case’ (<8 points) or ‘case’ ( 8 points). The K statistic to measure the rating agreement among the 3 interviewers was 0.79 (z = 11.13, p < 0.001), which was an acceptable level (‘substantial’ is the category below ‘almost perfect’ according to the classification system of Landis and Koch).7
Discussion
Other SRQ 20 validation studies have found that test sen-sitivity ranges from 63% to 90% and specificity ranges from 44% to 95%.3 The sensitivity of 73% and specificity of 82% in the current study is approximately midway between these ranges. The current study’s area under the ROC curve (0.84) compares favourably with a validation of the SRQ 20 in Brazil using the ROC (0.9).6 This means that the validity of the SRQ 20 is acceptable in Vietnam as assessed against in-depth psychiatric interviews. The inter-rater reliability K score of 0.79 suggests that the SRQ 20 is also acceptable.
Interest in mental health in Vietnam is slowly growing. With a major focus by the Vietnamese national government and international donors on poverty reduction, it is likely that the association between poverty and mental health will be recognised.8 If that happens, the need for valid, reliable, cheap, and easy-to-administer methods of measuring men-tal health at the community level will increase. The use of the SRQ 20 in Vietnam is recommended, using a cut-off point of 7/8 to determine cases.
Acknowledgements
The authors would like to thank Professor Dang Phuong Kiet who performed the in-depth psychiatric assessments for this study, and Professor Jair de Jesus Mari of the De-partment of Psychiatry, Escola Paulista de Medicina, Sao Paulo, Brazil, and Professor Martin Prince of the UK Insti-tute of Psychiatry, UK, for their advice and inspiring research. Tran Duc Thach of RTCCD, Vietnam, provided excellent data analysis support.
References
- Falkingham J, Namazie C. Measuring health and poverty. London: Health Systems Resource Centre; 2002.
- Harpham T, Reichenheim M, Oser R, et al. How to do (or not to do) series: measuring mental health in a cost-effective manner. Health Policy Plann 2003;18:344-349.
- World Health Organization. A user’s guide to the self reporting ques-tionnaire (SRQ). Geneva: World Health Organization; 1994.
- Tuan T, Lan PT, Harpham T, et al. Young Lives — an international study on child poverty. Vietnam — preliminary national report 2002. Hanoi: RTCCD-SC/UK Hanoi-GSO; 2003.
- National Centre for Social Services and Humanities. Human develop-ment report Vietnam. Hanoi: National Centre for Social Services and Humanities; 2001.
- Mari JD, Williams P. A validity study of a psychiatric screening questionnaire (SRQ-20) in primary care in the city of Sao Paulo. Br J Psychiatry 1986;148:23-26.
- Landis JR, Koch GG. The measurement of observer agreement for cate-gorical data. Biometrics 1977;33:159-174.
- Patel V. Poverty, inequality and mental health in developing countries. In Leon D, Walt G, editors. Poverty, inequality and health. Oxford: Oxford University Press; 2001:247-263.