J.H.K.C. Psych. (1993) 3, 5-8
SPECIAL TOPIC: CHILD & ADOLESCENT PSYCHIATRY
Summary
The temperament characteristics of 20 children of psychoactive substance depen dent fathers were studied and compared with those of 119 emotionally disturbed children as well as with the general population norms. The children of addicted fathers were found to be generally low in rhythmicity, adaptability and distractibil ity. They also displayed negative emotionality, withdrawal and lower threshold of responsiveness as compared to the norms for general population. The differences were further enhanced on rhythmicity and distractibility in subjects whose parents had greater severity of substance dependence. Sex and birth order of the child, duration of exposure of child to father's drug abuse, degree of psychosocial dys function in the father, and depression in the mother did not show any significant relationship with the temperament characteristics of the children. This study high lights the usefulness and need for research in this area.
INTRODUCTION
Several studies in the past few years have shown that certain temperament traits measured in childhood are associated with an increased risk for psychiatric disorders in adolescence (Thomas and Chess, 1977) and young adult hood (Thomas and Chess, 1984). There is also evidence in literature to suggest that temperament deviations in child hood may increase the risk for alcoholism in adulthood (Tarter, Alterman and Edwards, 1985). High behavioural activity (Tarter et al., 1985; Jones, 1968) and other charac teristics such low as attention, high emotionality and low sociability (Tarter et al., 1985) appear to comprise features of vulnerability to alcoholism in boys. Tarter et al. (1990a) reported high activity level in biological offsprings of alco holics. These temperament deviations might indicate a be havioural-genetic marker for alcoholism.
Similar search for a behavioural marker for substance abuse in general had concerned researchers. However, there is hardly any literature on relationship between tem perament and substance abuse other than alcoholism. Tar ter et al. (1990b) in their study on substance abusing adolescents reported them to be distinguishable from nor mal controls on a variety of temperament dimensions, e.g., higher on activity and lower on flexibility, mood stability, eating rhythm, daily rhythm and task orientation. Since children of substance abuse parents constitute a high risk group predisposed to development of psychiatric disorder in general or substance abuse in particular, it would be worthwhile to explore into the temperament patterns of these children.
AIMS AND OBJECTIVES
The present study was carried out with the aim of ex amining whether (i) the temperament profile of children of addicts differs from that of normal children or of emotional ly disturbed children, and (ii) the children's temperament correlates with their parents' pattern of substance abuse (severity and duration), psychosocial dysfunction in the sick parent and depression in the well parent. This preliminary study had an exploratory descriptive study design.
MATERIAL AND METHOD
SUBJECTS
The index sample consisted of 20 children whose fathers were diagnosed as suffering from psychoactive substance dependence (not abuse) using DSM-III criteria (APA, 1980) attending the Drug De-addiction and Treatment Centre (DDTC}, Department of Psychiatry, Postgraduate Institute of Medical Education and Research, Chandigarh. The child had the following criteria for inclusion and exclusion:
Inclusion criteria:
- Age 5-15 years.
- Minimum exposure to parent's drug taking behaviour: 2 years, and the child staying with the parent for the best 1 year at least.
- Both parents staying with the
- Only one child per family was
Exclusion criteria:
- Substance abuse or mental retardation in index sub jects.
- Significant physical or mental illness in the mother.
- History of substance abuse in the mother.
INSTRUMENTS
- Malhotra's Temperament Schedule (MTS; Malhotra and Malhotra, 1988). This is based on, and measures, the nine temperament traits identified by Thomas, Chess and Birch (1968) in Hindi (the local and nation al language). It has satisfactory reliability and validity.
- Drug Taking Evaluation Scale (OTES) by Holsten and Waal (1980). This was chosen for assessing the sever ity of drug (or alcohol) taking behaviour in the form of global score (range of scores 4-36).
- Dysfunction Analysis Questionnaire (DAQ) by Pershad et al. (1985). This assesses psychosocial dysfunction due to illness in the social, vocational, personal, fami lial and cognitive spheres. The higher the score the greater is the dysfunction.
- Hamilton Depression Rating Scale (HORS; Hamilton, 1960) was used to assess the severity of depression in the spouse of the patient.
PROCEDURE
A consecutive sample of 20 male married substance de pendent persons (12 opioid addicts and 8 alcoholics) attending the DDTC for treatment was taken. Each one of these was asked to bring his child (if they fulfilled the criteria as described above) and wife. Child's temperament was assessed using the MTS. Child's father was adminis tered OTES and DAQ, and mother was assessed for de pression on HORS. Both the parents were interviewed to record the psychosocial and demographic data pertaining to the child (age, sex, birth order, family type) and duration and nature of drug habit in the fathers.
Temperament data were compared with the norms of temperament scores for general population and with those of emotionally disturbed children attending the Child Psychiatry Clinic of the Department.
RESULTS
The mean age of the index sample was 10 years (s.d. 3.5). Half of them were boys. Half were eldest sibs, the rest being second in birth order. Twelve came from nuclear family. The duration of exposure to father's drug addiction or alcoholism ranged from 5 to 15 years (mean, 10 years, s.d. 3.4).
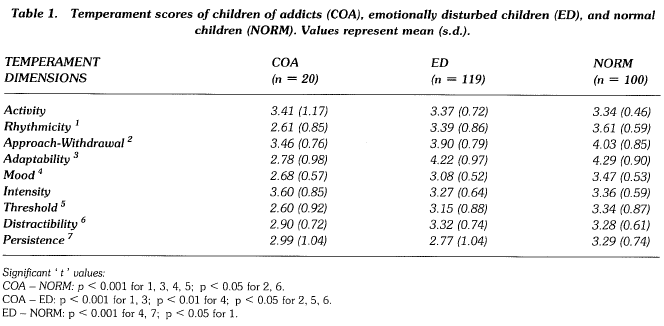
The table shows the temperament scores of the sample in comparison with normative data as well as with those of emotionally disturbed children.
The sample differed significantly from the norms in being lower on rhythmicity, approach-withdrawal, adaptability, mood, threshold of responsiveness and distractibility. When a similar comparison was made with the temperament scores of emotionally disturbed children, the differences persisted in all the above-mentioned temperament vari ables. The emotionally disturbed children themselves dif fered from the norms significantly only on rhythmicity, mood and persistence and not the others.
The temperament data of the sample were analysed across sex, birth order and duration of exposure to father's illness (upto 10 years versus more than 10 years) using unpaired 't' test. No significant difference emerged.
Regarding severity of abuse, the median score of 26 on OTES was used to categorize the patients as having moder ate (OTES global score upto 26; n = 11) or severs (OTES score more than 26; n = 9) degree of abuse. The tempera ment scores of the index sample were analysed across these two categories using unpaired 't' test. Children of se vere abusers were found to be significantly lower on rhyth micity and distractibility compared to children of moderate abusers. The mean and s.d. scores on rhythmicity of these two groups were, respectively, 1.98 ± 0.66 and 3.20 ± 0.36 (t = 4.79, df 18, p < 0.001). Similar scores on dis tractibility were 2.68 ± 0.12 and 3.65 ± 0.47 (t = 3.25, df 18, p < 0.01).
Finally, neither HORS scores in the mother (mild and moderate depression scores with cut-off at score 8; ten in each group) nor OAQ scores in the father (mild and moder ate-to-severe dysfunction with cut-off at 60%; 12 and 8 in the two groups respectively) were found to be significantly associated with any differences in the temperament scores of the children using unpaired 't' tests for the groups.
DISCUSSION
According to Buss and Plomin (1975), temperament be gins as inborn dispositions, subsequent course of which is determined by a complex interaction with the environment. Thus, it provides a unique window through which one may attempt to look into the nature-nurture intricacies involved in the genesis of substance use disorders. In the present study, children of substance dependent fathers were found to be lower in rhythmicity, less adaptible, having pro nounced negative emotionality, tending to withdraw in so cial situations, less distractible and having lower threshold of responsiveness as compared to normal children. These differences persisted when the former were compared with emotionally disturbed children, albeit the magnitude of dif ferences being smaller in this set of comparison. Only severity of substance abuse was associated with some tem perament dimensions, the children of fathers with severe degree of abuse being further low in rhythmicity and less distractible. Variables implicating potential environmental factors, such as duration of exposure of child to father's ill ness, dysf unction in father or depression in mother were not associated with the child's temperament profile.
In their review of temperament characteristics of children of alcoholics, Tarter et al. (1985) concluded that many of the temperament dimensions may be involved. Considering the six temperament factors extracted by Rowe and Plomin (1977), they discussed the role of activity level, attention span-persistence, emotionality, sociability and soothability as the factors with potential for further study in this high risk group. In their recent study using a scale derived from the traits identified by Thomas et al. (1968), they found adolescent drug abusers to differ significantly from the nor mal control on the following variables: general activity, fle xibility/rigidity, mood, eating rhythm, daily rhythm and task orientation (Tarter et al., 1990b). Factor analysis with vari- max rotation of the original scale scores yielded three orthogonal dimension: factor 1 (rhythmicity). factor 2 (moti vational and emotional propensities) and factor 3 (be havioral activity regulation). Significant differences were found between the substance abusers and the control group in case of the first two factors. Although using quite different methodology (with respect to both sample and in struments), the present study findings seem to be largely in line with these findings as well as with some of the earlier speculations (Tarter et al., 1985).
This preliminary study, as mentioned earlier, was ex ploratory in nature, and hence the findings need to be re plicated in different, larger and more specifically defined samples. For the present, however, it seems that the chil dren of addicts represent a particularly deviant group as far as certain temperament characteristics are concerned. Given the 'high-risk' background, one wonders if the study of temperament in this group might provide a way to understand how genetic predispositions may be translated into the risk behaviour patterns, as suggested by Tarter et al. (1985). Also, a deviant temperament profile in child hood often indicates higher vulnerability to psychopatholo gy later in life (Thomas and Chess, 1977, 1984), and the same may hold true in this group in question too. Finally, a deviant profile of temperament like the one found in the children of addicts makes parenting difficult. The difficulty is compounded by the fact that one of the parents may not be effective in the handling due to the problem of addic tion. Thus the issue of management and counselling of the parents with the aim of primary prevention in this high-risk category is also emphasized by this study.
It is not clear from existing literature to what extent the temperament profile of children of alcoholics might differ from that of children of drug addicts (non-alcoholic). Tem perament has been construed as both specific as well as a general risk factor (Malhotra, 1989). It may be worthwhile to study the temperament characteristics of children of alcoholics vis-a-vis drug addicts separately. The small sam ple size of the present study precludes any such meaningf ul comparison. It does, however, highlight the significance of temperament as a viable and promising perspective for in vestigating vulnerability to alcoholism and drug depend ence.
REFERENCES
American Psychiatric Association (1980) Diagnostic and Statistical Manual of Mental Disorders, 3rd ed. (Washington, D.C., APA Press).
Buss, A. & Plomin, R. (1975) A Temperament Theory of Personality Development (New York, John Wiley & Sons, Inc.).
Hamilton, M.(1960) A rating scale for depression, Journal of Neurology, Neurosurgery and Psychiatry, 23, pp. 56-62.
Holsten, F. & Waal, H. (1980) The OTES - Drug Taking Evalua tion Scale: a simple scale for the evaluation of drug taking be haviour, Acta Psychiatrica Scandinavica, 61, 273-305.
Jones, M.C. (1968) Personality correlates and antecedents of drinking patterns in adult males, Journal of Consulting and Cli nical Psychology, 32, 2-12.
Malhotra, S. (1989) Varying risk factors and outcomes: An Indian perspective, in: Carly, W.B. & McDevitt, S.C. (Eds.) Clinical and Educational Applications of Temperament Research (The Netherlands: Swets & Zeitlinger).
Malhotra, S. & Malhotra A. (1988) Malhotra's Temperament Schedule (Agra, National Psychological Corporation).
Pershad, D., Verma, S.K., Malhotra, A.K. & Malhotra, S. (1985) Measurement of Dysfunction and Dysfunction Analysis Ques tionnaire (Agra, National Psychological Corporation).
Rowe, D. & Plomin, R. (1977) Temperament in early childhood, Journal of Personality Assessment, 41, 150156.
Tarter, R.E., Alterman, A.I. & Edwards, K.L. (1985) Vulnerability to alcoholism in men: a behavior-genetic perspective, Journal of Studies on Alcohol, 46, 329-356.
Tarter, R.E., Kabene, M., Escaller, E.A., Laird, S.B. & Jacob, T. (1990a) Temperament deviation and risk for alcoholism, Alco holism: Clinical and Experimental Research, 14, 380-382.
Tarter, R.E., Laird, S.B., kabene, M., Bukstein, 0. & Kaminer, Y. (1990b) Drug abuse severity in adolescents is associated with magnitude of deviation in temperament traits, British Journal of Addiction, 85, 1501-1504.
Thomas, A. & Cgess, S. (1977) Temperament and Development (New York, Nrunner/Mazel).
Thomas, A. & Chess, S. (1984) Genesis and evolution of behavior disorder: from infancy to early life, merican Journal of Psychiatry, 140, 1-9.
Thomas, A., Chess, S. & Birth, A. (1968) Temperament and Be havior Disorders in Children (New York Univerity Press).
Correspondence: Dr. Savita Malhotra, Additional Professor, Department of Psychiatry, P.G.I.M.E.R., Chandigarh - 160012, India.