J.H.K.C. Psych. (1993) 3, Spl, 17-21
ORIGINAL PAPER
SUMMARY
This study aimed to examine twenty – five thalassaemia major patients, 12 boys and 13 girls aged 9-15 years for the presence of depression. Twenty- five normal children, matched for age, sex and family, acted as the control. Individual interview was conducted on the patients, the control, and their patients. The interview of patients took place after blood transfusion. The Children’s Depression Scale (CDS) (Australia Council for Educational Research) was used for assessment of depression and the Hong Kong Wechsler Intelligent Scale for Children was used for their intelligence quotients ( I.Q.). Four patients were identified to be at risk for depression while none was found among the control (p< 0.05). Total depression score of these four when compared with twenty- one non- depressed patients showed significant difference in all the subsales, but no difference was seen in the “positive” scores. Patients as a group has normal I.Q. while sex and puberty had no effect on depression.
INTRODUCTION
Cooley's anaemia (B-thalassaemia major), an inherited disorder of the red blood cells, is not uncommon in the Hong Kong population (Li, Cheng & Low, 1987; McFadzean & Todd, 1964) _ Affected children usually present with severe anaemia before the first birthday, and their lives are being sustained by monthly blood transfusions. In the past such patients inevitably died in the second decade as a consequence of massive iron overload. Nowadays with effective iron chelation, prognosis has improved considerably; however the long term outcome remains to be seen.
Children with chronic illness and their family members are prone to the development of psychological problems. Tsiantis et al (1982) had noted depression as one of the four major reactions in families of patients with Bthalassaemia major. This was understandable since depression was one of the commonest psychological reactions seen in persons under chronic stress. The aim of our study was to assess the presence of depression in our patients suffering from thalassaemia major.
MATERIAL AND METHOD
The subjects in this study consisted of 25 patients, 12 boys and 13 girls, under the care of the Department of Paediatrics, University of Hong Kong, Queen Mary Hospital. Their age ranged from 9 to 15 years (mean 11.9 ± 1.6). All had been diagnosed to have B-thalassaemia major in their first year of life, and given monthly blood transfusion since; their haemoglobin (Hb) was maintained between 9 to 14 g/dl. In this hospital, patients stayed overnight for transfusion on weekdays, which required absence from schools. An equal number of normal healthy controls, recruited from the Boys and Girls Association in the Lai Tak Estate, Hong Kong, was matched for age, sex and social class, and none had history of chronic physical or mental illnesses.
The parent, usually the mother, was asked to supply background data on the family. The Children's Depression Scale (CDS) as described by Lang & Tisher (1978), was used in the assessment of our subjects, after it had been translated into the local dialect. This contained 66 items, 48 relating to features of depression and 18 to positive feeling; related items were grouped into eight subscales. A score was given to each item in the subscale and the sum total of the first six subgroups was the "depression" score while the last two was the "positive" score. The following describes briefly the contents of the eight subscales:
1) Affective response: statements referred to the feeling and mood of the respondent (8 items)
2) Social problems: statements reflected the difficulties encountered in social interaction, feelings of isolation and loneliness (8 items)
3) Self-esteem: statements referred to the child's attitudes, concepts and feeling in relation to his own worth and value. (8 items)
4) Pre-occupation with own sickness and death: statements referred to the child's dreams and fantasies in relation to his disease and to death. (7 items)
5) Guilt: contents reflected the child's self blame (8 items)
6) Miscellaneous D items: this included depressive statements which could not be grouped with any of the above. (9 items)
7) Pleasure: referred to the presence of fun, enjoyment and happiness in the child's life, or to his capacity to experience them. (8 items)
8) Miscellaneous P items: included items not included in (7). (10 items)
The patients were interviewed individually in a quiet room, by one of the co-workers (A.C.). All interviews were conducted after patients had received blood transfusion with haemoglobin over 12 g/dl. Each of the 66 statements was written on a small card which was numbered. Five paper boxes were placed on the table and marked with different label as indicated below: (1) very right; (2) right; (3) not sure; (4) wrong; (5) very wrong. During the interview each of the 66 cards was presented to the patient in a predetermined order, and A.C. made sure the former understood the content. The patient was then asked to drop the card into the box which best represented his or her feeling on each statement. Scores from 1 to 5 was given to each answer. For a statement positive for depression, 5 scores were awarded if the answer was (1) very right, 4 scores for (2), 3 scores for (3), etc. For a statement negative for depression, the reverse took place. At the end of the interview, the patients were asked to comment on the session. The duration of this interview varied with the individual since each was allowed to proceed at his or her own speed. The same procedure was carried out with the control group.
A simple questionnaire had also been devised to seek information on parental age, occupation, number of offsprings and the nature of family structure (nuclear or extended). These data were obtained by interviewing parents of patients, and in the control group, by telephone contact. The manual of Hong Kong Wechsler Intelligent Scale for Children (WISC) was used (Hong Kong Government 1981) in assessing the intelligence quotient (I.Q.) of the patients.
A score two standard deviations above the mean depression score of the normal control was considered to be suggestive of depression.
The U.K. Registrar General's Classification of Social Class by father's occupation (1966) was used to assign social class.
Student's t-test and Chi-Square were used in the analysis of data.
RESULTS
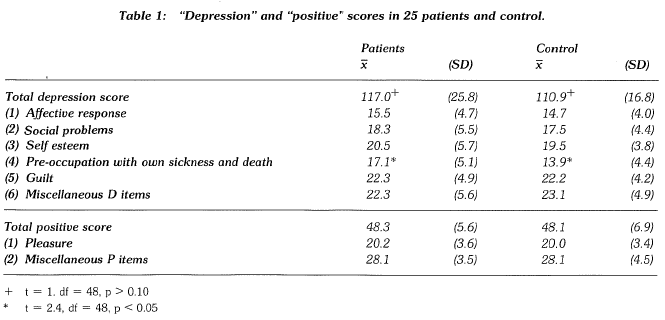
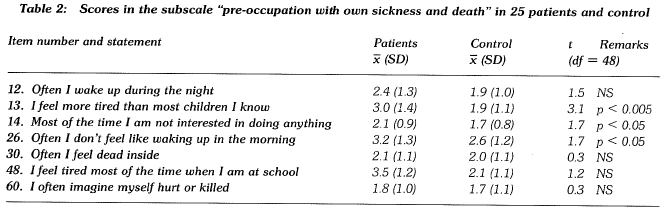
Patients had higher "mean depression score" than the control, but the difference was not of statistical significance (table 1). The higher scoring on one subscale "preoccupation with own sickness and death", which was of statistical significance, was attributed to higher marks on three of the seven statements (table 2). The "positive" score was almost identical in the two groups (table 1).
In the experimental group, no sex or age difference could be demonstrated in both the "depression" and "positive" scores (table 3).
Four patients had depression scores above 144.5 (i.e. two S.D. above the mean of the control in table 1) while none was found in the control group. Chi Square test showed this to be of significance (p < 0.05).
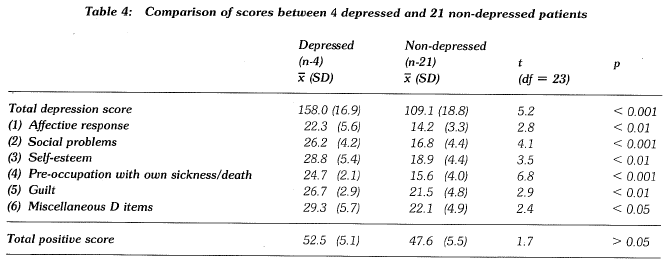
Table 4 compared the scores of the four "depressed" patients with twenty-one "non-depressed" ones; a significant difference was seen in all "depression" subscales, but not in the "positive" scores. Also, the mean scores of the latter 21 was almost identical with that found in the control (table 1).
The mean intelligence quotient of the patients was 100.5 (table 5). 19 patients were attending primary school compared with 16 controls but this was not of statistical significance.
Patients came from families with more siblings than the control (table 6). Fifteen patients and fourteen controls were the eldest in the family; nine patients have siblings similarly affected. Twenty one patients and twenty in the control group came from families of social class lII and the overwhelming majority (22 patients/21 control) came from nuclear families. The parental ages were similar in both groups (fathers and mothers of patients 43.7 ± 10.4, 37.8 ± 5.0 years; that of controls, 44.9 ± 11.3, 37.9 ± 4.4 years).



DISCUSSION
The assessment of psychological problems in the chronically ill patients is not an easy task because most established methods of measurement had derived from studies done on patients with primary psychiatric illnesses. The CDS used in this study also standardized on children suffering from depression (Lang, Tisher 1978). More recently Kazdin (1987) in his preliminary evaluation of the CDS, found that the depression scores correlated well with other depressive measures in his sample of hospitalized children and their parents.
In this study, the experimental group did not score significantly higher in the total depression score when compared with the control. However, a difference was seen in the subscale "pre-occupation with own sickness and death" (p < 0.05, table 2) which included three statements with higher scores: "I feel more tired than most children I know", "most of the time I am not interested in doing anything", often I don't feel like waking up in the morning". Students' I-test showed a statistical significance in all three (table 2, p < 0.05). These findings could be attributed to symptoms of depression, but in the absence of demonstrc1ble differences in the other subscales, and the possibility that this could be the effect of falling Hb level, a definite conclusion could not be drawn.
Lang & Tisher (1978) reported in their study of Australian children that the mean depression score in the "normal, clinical, and depressed" children were 116.9, 134.5 and 157.0. Our control group gave a mean depression score of 110.9 (table 1) which agreed well with the normal of the above. We considered a score, higher than 144.5, i.e. two standard deviations above the mean score of our normal control as being suggestive of depression. When the individual scores of the 25 patients were examined, four patients, (two boys and two girls) showed depression scores which were above 144.5 and all were over 10 1/2 years; none was found in the control group. Chi-Square test showed this to be of significance (p < 0.05). When the scores of the four "depressed" patients were compared with the 21 "non-depressed" group, a significant difference was seen in all the depression subscales, (table 4). Although at the time of study, no psychiatric interview had been conducted on them, they should be considered to be at risk for depression and needed further assessment, and possible treatment.
We were not able to single out any characteristic feature from the "depressed" patients which distinguish them from the "non-depressed". On comparing the "positive" scores of both groups, no significant difference could be found (table 4). Apparently the "depressed" patients had a normal ability to seek pleasure and enjoyment, which is a point to be remembered when treatment is being planned. Further study is indicated to better define the risk factors for depression in these patients.
Rutter (1986) found a higher incidence of depression in post-pubertal children, and he attributed this to the physiological changes that took place. This study did not find a positive correlation between patients' age and the depression score (table 3), possibly due to the small sample size; also among our patients, puberty was either absent or markedly delayed (Li, Cheng & Low, 1987), making it difficult to define the onset of puberty. Sex was not found to be a positive correlating factor (table 3). In the IQ assessment of patients, they were found to be in the normal range. The frequent absence from school could have adverse effect on their schooling.
The 1981 Hong Kong WISC had been standardized after testing 1100 local school children. It was not repeated on the control in the study.
Information obtained confirmed that the family background was comparable in both groups*.
CONCLUSION
As a group, patients with Cooley's anaemia showed a higher depression score which was not of statistical significance when compared with the control. However on closer scrutiny, four patients, with none in the control, had total depression scores greater than 144.5 and were considered to be at risk for depression. Comparison of the four "depressed" with the 21 "non-depressed" patients showed significant difference in the scores of all the depression subscales, but there was no difference in the "positive" scores. Age and sex, did not appear to be positive correlating factors. Since patients did not have normal puberty, it is difficult to confirm a higher incidence of depression in postpubertal patients. No single characteristic had been found to account for the above. Further study was indicated to better identify the underlying factors for depression in our patients.
CONCLUSION
This study was supported by the Research Grants from the Medical Faculty Funds and the Wu Chung Medical Research Fund, Hong Kong University.
REFERENCES
Kazdin, A.E. (1987) Children's depression scale - Validation with child psychiatric inpatients. Journal of Child Psychology & Psychiatry, 28, 29-41.
Lang, M. & Tisher, M. (1978) Children's Depression Scale. The Australian Council for Educational Research Limited.
Li, A.M.C., Cheng, M.Y. & Low, W.D. (1987) Growth and developmet in patients with homozygous B-thalassaemia in Hong Kong. Thalassaemia: pathophysiology and management Part A. Fucharoen, S. Rowley, P.T. & Paul, N.W. (eds). March of Dimes. Birth Defects: Original Article Series 23; 23:5A, 441- 448.
Manual of Hong Kong Wechsler Intelligence Scale for Children(l981). Hong Kong Government.
McFadzean, A.LS. & Todd, D. (1964). The distribution of Cooley's anaemia in China. Transactions of the Royal Society of Tropical Medicine and Hygiene.
Rutter, M. (1986) Issues and perspective in depression in young people. In: Rutter, M., Tizard, C.E. & Read, P.B. (eds.) Developmental and Clinical Perspectives. Guilford Press.
Tsiantis, J., Xypolita-Tsantili, D. & Papadakou-Lagoyianni, S. (1982) Family reactions and their management in a parents group with beta-thalassemia. Archives of Disease in Children 57:860-863.
*Chung See Yuen MBBS, MRCPsych. Senior Lecturer, Department of Psychiatry, University of Hong Kong.
Anita Li Ming Cheng MBBS, FRCP (Edin), OCH (London). Senior Lecturer, Department of Paediatrics, University of Hong Kong.
Angela Cheung Man Wei B.A. Research Assistant, Bryn Mawr College, USA.
*Correspondence: Department of Psychiatry, Queen Mary Hospital, Pokfulam, Hong Kong.