Hong Kong J Psychiatry 2001;11(4):9-16
ORIGINAL ARTICLE
Tina M Ng-Tse
Dr Tina M Ng-Tse, PhD, Director, Postgraduate Studies, School of Nursing and Midwifery, Curtin University of Technology, Perth, Australia
Address for correspondence: Dr Tina M Ng-Tse, PhD, Director, Postgraduate Studies, School of Nursing and Midwifery, Curtin University of Technology, GPO Box U1987, Perth, Western Australia 6845
Tel: (61 8) 9266 2753; Fax: (61 8) 9266 7485
E-mail: T.Tse@curtin.edu.au
Submitted: 27 April 2001; Accepted: 09 August 2001
Abstract
The Impact of Mental Illness questionnaire is designed to quantify attitudes towards and experience with mental illness of young Chinese women. To ensure a high level of content and face validity, items for the questionnaire were generated from semi-structured interview transcripts and judgement was sought from an expert panel. Scores obtained from 111 young Chinese women with schizophrenia were used to demonstrate the reliability of the instrument. The 60-item, 5-point Likert scale is operationalised by 5 variables: prospective marriage, the illness experience, occupational role functioning, family relations, and social relations. Psychometric properties of the scale were found to be reliable and internally cohesive.
Key words: Chinese, Women, Mental illness, Questionnaire
Introduction
Chronic mental illness often results in profound alterations in the ways in which affected persons experience themselves and others, and thus strikes at the core of the individual’s psycho-socio-educational integrity. It has been acknowl- edged that the psychosocial aftermath of an episode of schizophrenia or affective disorder, even when the acute symptoms of the disorder are successfully treated, can change the expectations of the affected person and lead to role disablement and a marked decrease in personal achieve- ment and social recognition.1-9 Culturally determined val- ues and beliefs are likely to play an important part in the manifestation and course of mental illness10-12 and may af- fect psychosocial functioning and shape the illness experi- ence of the person. A variety of culturally patterned strate- gies used by individuals in response to crises such as acute or disabling illness has been examined.13-21 For example, under the influence of the doctrine of Confucianism and Taoism, Chinese people tend to exhibit ‘f atalistic voluntarism’ (a mixture of fatalism and activism)22 with re- gard to the causation of mental illness and have a stronger belief in external control23-27 than their Western counterparts.28 Given people’s different socio-cultural environments, the reactions of individuals affected with psychosis are likely to vary considerably in the extent to which they success- fully ameliorate inevitable effects, and shape the outcome of and adjust to a severe mental illness and its accompanying disabilities.
The way in which young women cope with and adapt to illnesses such as schizophrenia remains largely unexplored and unknown. In order to investigate the effect of illness on social structures (e.g. family, workplace, illness experience, female role identity, and ways of coping), a new assessment instrument for young Chinese female patients is deemed necessary.
Objective
The purpose of this study was to develop a measuring tool, ‘Impact of Mental Illness’ (IMI), to elicit information on patterns of illness experience, psycho-socio-occupational role functioning, and views on marriage exhibited by young Chinese women with a severe mental illness such as schizophrenia.
Methods
Item Generation
Questionnaires are commonly used in research. The measurable and objective outcomes can help to verify and establish facts and f indings that may be generalisable for other populations. However, the use of a rating scale has been criticised for lacking sensitivity and failure to capture the essence of the phenomenon being studied. In order to construct a questionnaire that is representative of a true picture of young Chinese women’s experience of living with a mental illness, semi-structured interviews were conducted to generate a pool of items to form the basis of the IMI questionnaire.
Thirty female patients attending the psychiatric out- patient clinics of 2 research centres in Hong Kong and Shenzhen, China, consented to a 30 to 45 minutes tape- recorded semi-structured interview. These women were aged between 22 to 31 years, had schizophrenia for the past 2 to 5 years without a history of substance misuse, and were mentally stable.
It was presumed that the women could express their feelings and thoughts in the interview and that the analysis of their descriptions would reveal the essential information of their experience with schizophrenia. Data generated from the 30 interview transcripts provided valuable insight into the complexity of the women’s experience. This en- abled the construction of the questionnaire in specific direc- tions to examine the women’s response to the 5 domains (prospective marriage, the illness experience, occupational role functioning, family relations, and social relations) of the study.
The wording of the questionnaire items was written in the way that the women expressed themselves during the interviews. The f irst draft of the questionnaire was submit- ted to a panel of judges considered to be experts in the field of social psychiatry. They were asked to indicate their level of agreement with the scope of the items and the extent to which the items reflect the concepts under consideration. As a result, some items were removed and several items were modified in accordance with comments from the panel judges.
The content and face validity of the questionnaire was then conf irmed. In order to ascertain clarity, readability, sensitivity, and clarity of the items, the revised version of the questionnaire was administered to 4 young women with a severe mental illness. The women were told that they could stop at any time to discuss any queries with the researcher who would make notes when there were signs of doubt or hesitation in answering an item or if it took a long time to complete a question. On completion of the questionnaire, the women were asked for feedback on their understanding of the questionnaire and its directions, or if they had found certain statements objectionable in any way. Consequently, revisions and refinements were made in order to eliminate problems encountered during the trial. The questionnaire was edited once more and then reproduced for f inal administration.
Patients
In order to collect a suff iciently large number of women to allow a principal component analysis to be conducted, all young women aged between 18 to 36 years, who were resident in Hong Kong or Shenzhen for no less than 5 years, with not more than 10 years history of schizophrenia, no history of substance misuse, attending the outpatient clinics in the 2 research locations, and mentally stable, were invited to participate in the study. The questionnaire was given to 135 women, and 110 returned the completed form (response rate, 81.5%). The mean age of the women was 27.5 years (SD, 4.73 years; range, 18-36 years). Seventy seven percent of the women were single, 18% were married and 5% were divorced. Approximately half of the women had suffered from schizophrenia for 5 to 9 years. About 25% of the women had no history of admission to hospital but 15% had been admitted 3 or more times. The majority of the women completed secondar y or post-secondar y education. Fewer than 10% of the women completed pri- mary education only. Sixty f ive percent of women were employed and approximately 90% worked full time; 25% were unemployed, and the remainder were either engaged in full time study or home duties.
Statistical Procedures
The psychometric properties of the IMI questionnaire were analysed using the Statistical Package for the Social Sciences (SPSS) as follows:
- Factor analysis of the variables of the IMI was performed using the principal component method with varimax rotation in order to examine correlations among items. Missing data were replaced by mean values.
- Conf irmation of the unidimensionality of the scale/ subscale structure was achieved using the multitrait scaling analysis. Those items showing item-total correla- tions of less than 0.30 would be rejected. However, if item- total correlations were found to be too high (approximately 0.70), they were considered to be redundant and there- fore not complementary to each other, and would also be rejected. In addition, the value of Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy should be greater than 0.6 and the Bartlett Test of Sphericity should be significant.
- Coefficient alpha was used to estimate the degree to which the sub-scale had internal consistency. The magnitude that a reliability coeff icient must achieve will vary according to the purpose for which the test scores will be used. Since the measure was used as a basis for group comparisons, coeff icients in the vicinity of 0.60 to 0.70 were consid- ered sufficient.
Results
Generation of the Questionnaire
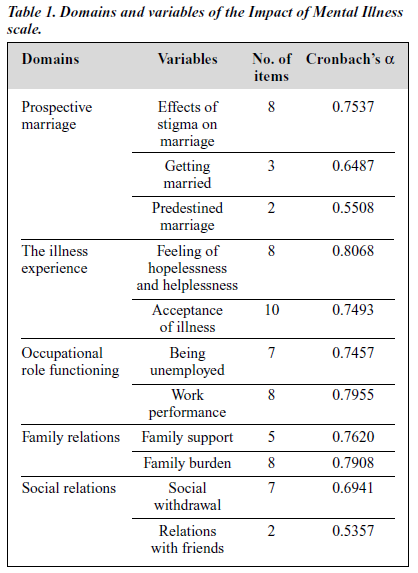
Each concept of the IMI questionnaire was tested separately in accordance with the guidelines stated above. As a result of a series of data analysis of the questionnaire, 60 attitude items on which the subject expressed the degree of agree- ment on separate 5-point scales (totally agree, agree, partly agree and partly disagree, disagree, and totally disagree) are included in the questionnaire. The questionnaire contains 5 dimensions of opinion on the effects of mental illness on a young woman’s life. The 5 domains are: prospective marriage, the illness experience, occupational role functioning, family relations, and social relations (Table 1). Details of the construction of the 5 domains (subscale) of the questionnaire are presented as follows.
Prospective Marriage
Three variables labelled as ‘effects of stigma on marriage’, ‘getting married’, and ‘predestined marriage’ are included in the subscale that addresses the perceptions and concerns of a young woman with mental illness on her prospective marriage.
Effects of Stigma on Marriage
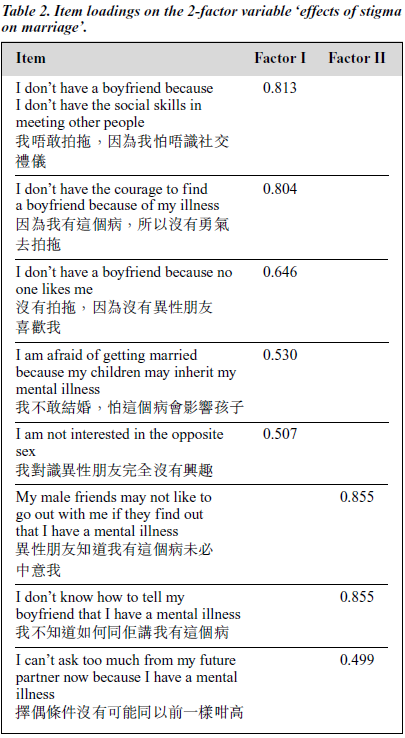
The variable ‘effects of stigma on marriage’ is operation- alised by 8 items. These items represent the effects of negative images of mental illness that prevent a woman from having a fair chance of looking for the right partner. As a result, criteria for selection of a marriage partner might have lowered substantially.
Internal consistency for the variable was examined using Cronbach’s alpha. It was found that the item cor- relations for the items were all above 0.30. The coeff icient alpha was 0.75. The 8 items for the variable were subjected to principal components analysis based on the derived cor relation matrix. The solution indicated the existence of 2 factors with eigenvalues greater than 1. The 2-factor solution accounted for 54% of the total variance and each factor has approximately half the considered variance. The 5 items for factor I reflect the negative self-perception in relation to prospective marriage as a result of having mental illness. The 3 items for factor II concern the dilemma of disclosure of the woman’s mental health status to a prospective partner for fear of rejection (Table 2).
Views on Getting Married
The 3-item variable ‘getting married’ represents the young and liberal generation of females who believe that one should not get married too young as enjoying life should be a priority. A principal component factor analysis with varimax rotation found that the solution could not be rotated and the factor analysis indicated that only 1 component was extracted. The interscale correlations solution showed that the correlation of each item was high (>0.40) [Table 3]. The internal consistency of the variable was satisfactory (a = 0.65).

Predestined Marriage
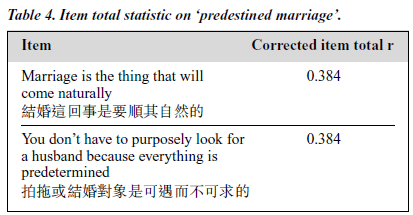
The 2-item variable ‘predestined marriage’ reflects that marriage is part of one’s predetermined life script. The 2 items had a satisfactory item correlation of 0.384 (Table 4) but the coefficient alpha (0.55) was relatively low.
Married Women’s Views on Their Marriage
The 2 variables, ‘family dynamics’ and ‘impact of illness on marriage’, of this subscale were designed to investigate the married women’s perceptions of their roles as house- wives and of their relationships with their husbands. It also attempted to explore the effects of the illness on their marriages. However, only 15 married women completed this part of the questionnaire. As a result, the KMO measure of sampling adequacy was below 0.6, and Bartlett’s Test of Sphericity was 0.014. Therefore, no further analysis was conducted.
The Illness Experience
This domain consists of 2 components (feelings of hope- lessness and helplessness, and acceptance of the illness) that attempts to identify the women’s experience with their illness.
Feelings of Hopelessness and Helplessness
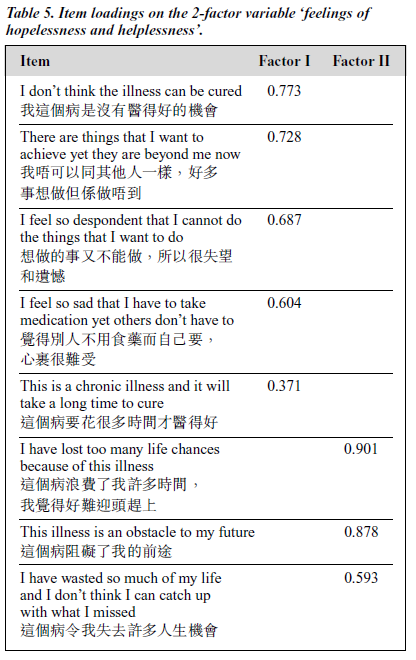
The 8 items on variable ‘feelings of hopelessness and help- lessness’ represent a negative perception towards the course of the illness and its negative impact on life chance, reflect- ing a pessimistic view towards the illness.
The outcome of a reliability analysis of the items indicated that all items had good cor rected item-total correlations. The Cronbach’s alpha for the overall scale was 0.81. Two factors were identif ied by the scree plot of eigenvalues. Both the factors accounted for half the consid- ered variance. Factor I consisted of 5 items that represent a pessimistic view on the prognosis of the illness. The 3 items for factor II relate to the effects of the illness on loss of opportunities for exploring life as a young woman. Overall, the variable reflects the feelings of hopelessness and help- lessness because of the effects of mental illness (Table 5).
Locus of Control
Items on variable ‘locus of control’ reflect the belief that the illness is part of the predetermined script of one’s life — that confrontation of the illness is unnecessary and that one should conform with the treatment regimen and that out- comes of one’s illness are out of one’s control, thus leaving everything in the hand of fate. Yet at the same time one should face the reality and do whatever one could to strive to improve. It is unfortunate to suffer from mental illness, but many people are worse off.
Initially, the variable had 11 items. After examining the magnitude and direction of the relationship among the items, 1 item was found to have a low level of item-scale correlation. The misf it item was removed in the subsequent analyses of the scale. The result indicated that the remain- ing 10 items would be effective for discriminating the de- gree in measuring the underlying concept, that is, accep- tance of the illness. The Cronbach’s alpha of 0.75 was con- sidered to be satisfactory. The 2 underlying concepts of the
variable were confirmed by the factor analysis. Each factor accounted for half of the considered variance. The 6 items in factor I and 4 items in factor II projected a positive attitude of the individual in handling the illness situation (Table 6).

Occupational Role Functioning
Under the section ‘occupational role functioning’, there are 2 separate components — 1 is for those who are currently not involved in a paid job and another is for income earners who are working either full time or part time. Women who are involved in full time home duties or in full time study were not required to complete this section.
Being Unemployed
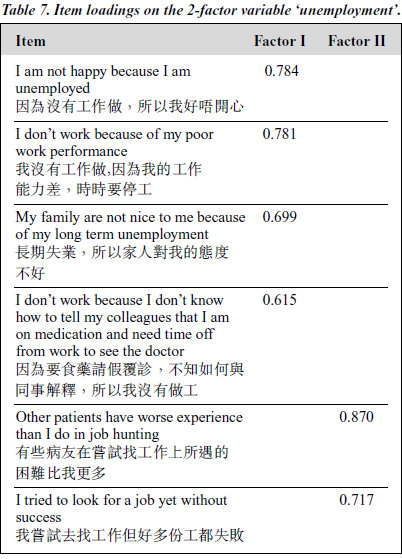
The 7-item variable relates to negative experiences of being unemployed. The Cronbach’s alpha for the overall subscale was equal to 0.75. The varimax rotation produced 2 factors that had eigenvalues of more than 1.00 accounting for 62% of the variance of the standardised items. The vari- ances accounted for by the 2 factors were 36.91 and 24.90, respectively. The 4 items for factor I reflect the negative consequences of mental illness on an individual’s inability to perform a paid job. The 2 items for factor II represent the experience of unsuccessful job seeking (Table 7).
Work Performance
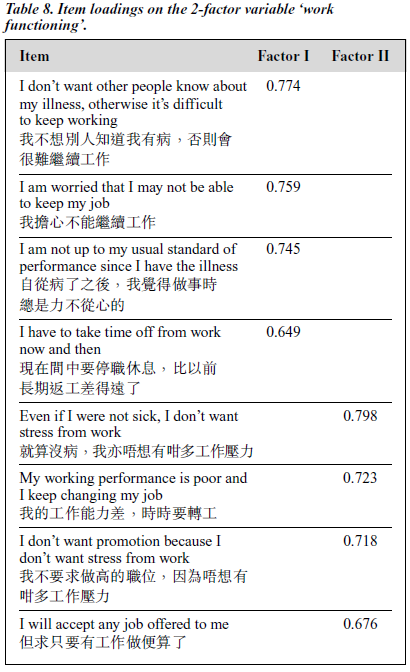
The 8 items for the variable ‘work performance’ relate to the impact the illness has on job performance. There were 2 components with an eigenvalue of greater than one, account- ing for 58% of the variance. All items had a satisfactory level of corrected item total g. Internal consistency was also acceptable (a = 0.80). The 4 items for factor I provide a factual description of the self-perceived substandard work performance and the intention to conceal mental health status from peers in order to secure a job. Factor II also has 4 items, which reflect a non-competitive attitude towards career development (Table 8).
Family Relations
The 14 items for the domain ‘family relations’ are oper- ationalised by 2 variables, ‘family support’ and ‘family burden’, which represent ambivalent attitudes towards the family. The 6 items of the ‘family support’ variable relate to positive relations with the family, while the 8 items for the ‘family burden’ variable reflect a perceived negative reception from the family.
Family Support
The acceptance by the family projected by this variable is one that emphasises unconditional caring attitudes and f inancial support from the family. Initially, there were 6 items in the variable ‘family support’. An examination of the items comprising the variable indicated that 1 item had a low (0.2388) corrected item-total correlation suggesting that it was a misfit item, therefore the item was deleted. The other items were sufficiently high (0.37 to 0.61) to measure the same concept without being redundant. The Cronbach’s alpha was raised from 0.7378 to 0.7620, which again justified the decision to remove the misfit item. Two factors were generated from the factor analysis: the eigenvalues were 2.113 for the first factor and 1.754 for the second. The percentage of variance explained by each factor was 35% and 29%, respectively. The 3 items for factor I represent appreciation of the family support. Factor II consists of 2 items in each of which the wish for better communication that promotes understanding is emphasised (Table 9).

Family Burden
The 8 items for the variable ‘family burden’ represent a neg- ative orientation towards the interdependent relationship with the family, the traditional Chinese family values inter- relatedness of its members — an individual is expected to share the family resources as well as to contribute to the wellbeing of the family and failing to meet this obligation might result in guilt and shame.
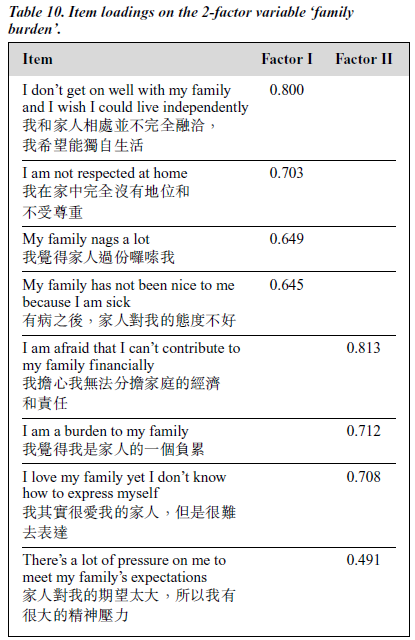
The extent to which the set of items measured the same dimension of the construct was investigated. Cronbach’s coeff icient was 0.79. The correlations of each item with the variable ranged from 0.37 to 0.62, which indicated that the items adequately measured the underlying concept. The 2- factor solution accounted for 54% of the total variance. The percentage of variance explained by each factor was 28.057 and 25.836, respectively. The first factor comprises 4 items concerning negative self perception for being unable to con- tribute and to meet with the family’s expectations. The 4 items for factor II relate to negative receptions received from family (Table 10).
Social Relations
‘Social relations’ is operationalised by 9 items. The 7-item vari- able, labelled as ‘social withdrawal’, represents a restrictive social interaction which could either be related to disinterest in making friends or else to feelings of inferiority because of having mental illness. The other 2 items reflect a positive relationship with friends and is named ‘relations with friends’.
Social Withdrawal
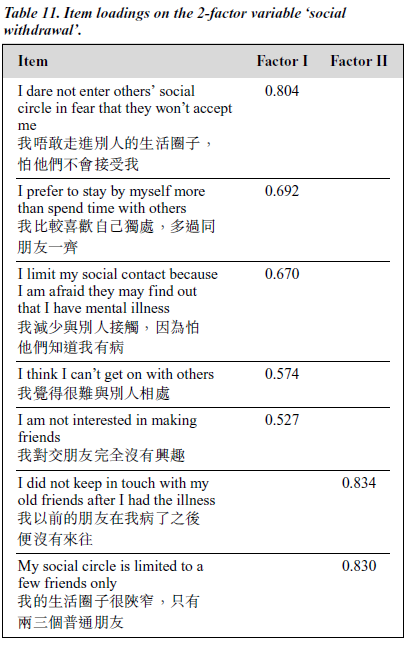
The 7-item variable ‘social withdrawal’ focuses on social avoidance behaviours that lead to a restrictive social circle. Social withdrawal behaviours could be related to the label- ling effect of mental illness and/or simply that the person prefers to spend time by herself than spending time with others. The interscale correlation solution showed that the correlation of each item ranged from 0.35 to 0.52. The co- eff icient alpha was 0.69. There were 2 components with an eigenvalue of greater than 1. The distribution of the eigen- values suggested that factor I had the largest eigenvalues (2.2) and accounted for 31.6% of the total variation. Factor II had 1.5 and accounted for 21.5% of the variance. Factor I comprised 5 high loading items, all of which concerned social avoidance. The 2 items for factor II gave a factual description of limited social circle (Table 11).
Relations with Friends
The 2 items for the variable ‘Relations with Friends’ relate to positive relationships with friends. Outcome of a re- liability analysis of the items indicated that the 2 items had a satisfactory corrected item-total correlation (0.3663) [Table 12]. The Cronbach’s alpha for the overall scale was equal to 0.54, which was considered to be low.
Conclusion
Psychiatric disability has a far-reaching impact on the sense of mastery, role functioning and commitment for a person with a severe mental illness. Culturally determined values, beliefs, and gender-specif ic expectations may have differ- ent levels of tolerance and stigmatisation, and support or reinforce different patterns of coping with the illness, which in turn affect the person’s opportunity for personal achieve- ment and social recognition. When there is no apparent im- mediate measure that can free people with severe mental illness from psychiatric symptoms, they must attempt to learn to live with the illness.
The IMI is a 60-item, 5-point Likert scale, self-completion questionnaire developed to elicit patterns of the perception of illness experience and role functioning of young Chinese women with a mental illness such as schizophrenia. The content of the scale items and ideas for item wording were generated from interview data so as to ensure the question- naire adequately reflects the complexity of a woman’s attitudes, beliefs, and experience of a severe mental illness and its effects on her life. Scale items were categorised to 5 domains — prospective marriage, the illness experience, occupational role functioning, family relations, and social relations. Due to a lack of statistical power to comprehen- sively analyse the data for married women, the domain ‘effect of illness on mar riage’ was excluded from the analysis. The principal components analyses suggested sub- categories within each domain appear theoretically relevant to Chinese culture and psychosocially to young Chinese women with a severe mental illness. In terms of psycho- metric properties, adequate variance in scores has been demonstrated. Although the coeff icient alpha for the 2 subscales of predestined marriage and relations with friends were relatively low. However, given the fact that alpha (0. 55 and 0.54, respectively) were obtained with only 2 items, the Spearman-Brown formula would predict that were there to be a moderate increase in test length contemplated (say 6 items), the alpha would increase substantially. With respect to future use of the variables ‘predestined marriage’ and ‘re- lations with friends’, it would be benef icial to construct a few more linking items to cover a wider perimeter of the underlying construct and to achieve a better reliability coeff icient. Overall, the content validity and reliability of the instrument have been established. At the time the ques- tionnaire was developed, it was conceived as a potentially effective instrument for reflecting a young Chinese woman’s perception and experience of living with a severe mental illness such as schizophrenia. However, further studies need to be done to determine the questionnaire’s test-retest reli- ability and its generalisability to other groups of women with mental illness who have a similar cultural background, for example Chinese women living in rural areas or overseas, or other Asian women. Studies should also be conducted to validate the variables on effects of a mental illness on a married woman’s relationship.
References
- Seeman MV. Women and schizophrenia. Medscape Women’s Health [Serial online] 2000; 5(2). Available from:http://www.medscape.com/medscape/WomensHealth/journal/2000/v05.n02/wh7146.seem/wh7146.seem-01.html. Accessed April 11, 2000.
- Craig T, Fennig S, Tanenberg-Karant M. Six-month clinical status as a predictor of 24-month clinical outcome in first admission patients with schizophrenia. Ann Clin Psychiatry 1999;11:197-203.
- Lee PW, Lieh-Mak F, Wong MC, Fung AS, Mak KY, Lam J. The 15- year outcome of Chinese patients with schizophrenia in Hong Kong. Can J Psychiatry 1998;43:706-713.
- Harrow M, Sands JR, Silverstein ML, Goldberg JF. Course and out- come for schizophrenia versus other psychotic patients: a longitudinal study. Schizophr Bull 1997;23:287-303.
- Meise U, Fleischhacker W. Perspectives on treatment needs in schizophrenia. Br J Psychiatry 1996;168:9-16.
- Davidson L, McGlashan T. The varied outcomes of schizophrenia. Can J Psychiatry 1997;42:34-43.
- Hatf ield AB. Serving the unserved in community rehabilitation programs. Psychosoc Rehab J 1989;13:71-82.
- Weller MP. Mental illness — who cares? Nature 1989;339:249-252.
- Drake RE, Wallach MA, Hoffman JS. Housing instability and homelessness among aftercare patients of an urban state hospital. Hosp Comm Psychiatry 1989;40:46-51.
- Jablensky A. Schizophrenia in the third world: an epidemiological perspective. USA: Harvard Center for the Study of Culture and Medicine; 1993.
- Jablensky A. Course and outcome of schizophrenia and their prediction. In: Gelder M, Andreasen N, Lopez-Ibor J, editors. The New Oxford Textbook of Psychiatry. London: Oxford Press; 2000.
- Rahman M, Indran S. Disability in schizophrenia and mood disorders in a developing country. Soc Psychiatry Psychiatr Epidemiol 1997;32: 387-390.
- Anderson JM, Blue C, Lau A. Women’s perspectives on chronic illness: ethnicity, ideology and restructuring of life. Soc Sci Med 1991;33: 101-113.
- Middelboe T, Mortensen EL. Coping strategies among the long term mentally ill. Acta Psychiatr Scand 1997;96:188-194.
- May-Teerink T. A survey of rehabilitative services and people coping with physical disabilities in Uganda. East Africa. Int J Rehabil Res 1999;22:311-316.
- Collins ME, Mowbray CT, Bybee D. Measuring coping strategies in an educational intervention for individuals with psychiatric disabilities. Health Soc Work 1999;24:279-290.
- Shih FJ, Meleis AI, Yu PJ. Taiwanese patients’ concerns and coping strategies: transition to cardiac surgery. Heart Lung 1998;27:82-98.
- Brillhart B, Johnson K. Motivation and the coping process of adults with disabilities: a qualitative study. Rehabil Nurs 1997; 22:255-256.
- Aranda M, Knight BG. The influence of ethnicity and culture on the caregiver stress and coping process: a sociocultural review and analysis. Gerontologist 1997;37:342-354.
- McColl MA, Skinner H. Assessing inter- and intrapersonal resources: social support and coping among adults with a disability. Disabil Rehabil 1995;17:24-34.
- Doyle Y, Moffatt PC, Hoffman JS. Coping with disabilities: the per- spective of young adults from different ethnic backgrounds in inner London. Soc Sci Med 1994;38: 1491-1498.
- Lee R. Cultural tradition and stress management in modern society: learning from the Hong Kong experience. In: Lin T, Tseng W, Yeh E, editors. Chinese societies and mental health. Hong Kong: Oxford University Press: 1995:40-52.
- Ho D. Interpersonal relationships and relationship dominance: an analysis based on methodological relationalism. Asian J Soc Psychol 1998;1:1-6.
- Tseng W, Lu Q, Yin P. Psychotherapy for the Chinese: cultural considerations. In: Lin T, Tseng W, Yeh E, editors. Chinese societies and mental health. Hong Kong: Oxford University Press; 1995:281-294.
- Yang KS. Do traditional and modern values coexist in a modern Chinese society [article in Chinese]. Proceedings of the Conference on Chinese Perspectives on Values. Taipei: Centre for Sinological Studies; 1992:117-158.
- Yang KS. Chinese social orientation: an integrative analysis. In: Lin T, Tseng W, Yeh E, editors. Chinese societies and mental health. Hong Kong: Oxford University Press; 1995:19-39.
- Yang KS, Ho D. The role of yuen in Chinese social life: a conceptual and empirical analysis. In: Paranjpe A, Ho DYF, Rieber R, Asian contributions to psychology. New York: Praeger; 1988:263-281.
- Leung K. The role of beliefs in Chinese culture. In: Bond M, editor. The handbook of Chinese psychology. Hong Kong: Oxford University Press; 1996:247-262.