Hong Kong J Psychiatry 2003;13:12-15
ORIGINAL ARTICLE
Abstract
Objective: This study was performed to investigate the rate of occurrence, severity, and course of clozapine-induced thrombocytopenia.
Patients and Methods: This was a retrospective study of the case records of the 28 patients receiving clozapine therapy.
Results: Five patients (17.8%) had had at least one episode of thrombocytopenia. There were no differences in sociodemographic and clinical variables between patients who had and did not have thrombocytopenia. Analysis of the characteristics of thrombocytopenia revealed the episodic nature of the condition. All the thrombocytopenic episodes took place within the therapeutic dose range of clozapine and resolved without clozapine dose reduction.
Conclusion: Thrombocytopenia is not an unusual adverse effect of clozapine therapy. A prospective study with is required to confirm these findings.
Key words: Agranulocytosis, Clozapine, Leukopenia, Neutropenia, Platelets, Thrombocytopenia
Dr K Jagadheesan, MD, Central Institute of Psychiatry, Ranchi, India. Dr SK Agarwal, DPM, Central Institute of Psychiatry, Ranchi, India. Dr S Haque Nizamie, MD, DPM, Central Institute of Psychiatry, Ranchi, India.
Address for correspondence: Dr S Haque Nizamie, Central Institute of
Psychiatry, Ranchi-834 006, India.
Tel: (91 651) 232 209/232618, ext 242/212/243
E-mail: jagpsy@yahoo.com
Submitted: 11 July 2001; Accepted: 11 October 2001
Introduction
For the management of treatment-resistant schizophrenia, clozapine has superior efficacy to that of typical anti- psychotics.1 Recently, its beneficial effects in the man- agement of affective disorders are also being recognized.2 Commonly reported haematological adverse effects of clozapine include agranulocytosis, neutropenia, leuko- cytosis, and eosinophilia.3 Thrombocytopenia as a com- plication of clozapine therapy is seldom reported. A review of the database of the Clozaril Patient Monitoring Service (CPMS) of UK and Ireland showed that clozapine was discontinued due to thrombocytopenia in 6 of 6316 patients.4
Apart from this review, only a few case reports5, 6 con- stitute the existing pool of information regarding clozapine- induced thrombocytopenia. Thrombocytopenia can lead to several complications including dangerous cerebral haemorrhage.7 However, no studies have addressed this adverse effect of clozapine. Therefore, a pilot study was designed to investigate the rate of occurrence, severity, and course of clozapine-induced thrombocytopenia.
Patients and Methods
This retrospective study was conducted at the Central Institute of Psychiatry, Ranchi, India. In this tertiary level hospital, clozapine therapy is considered for patients who have had poor or no response to adequate trials of at least 2 antipsychotics, tardive dyskinesia, or prominent negative symptoms. For patients receiving clozapine, haematological examination is regularly performed using the Sysmex K-4500 haematology analyser (Toa Medical Electronics Co Ltd, Kobe, Japan). Haematological examination is done weekly for the first 3 months, fortnightly for the next 3 months, and monthly thereafter. The frequency of haemato- logical examination is increased to once per week, biweekly, or alternate days if any haematological abnormality is suspected. In this hospital, all the psychiatric diagnoses are made according to the ICD-10.8
This study was performed between March and April 2000. The inpatient population (n = 380) was screened to identify patients receiving clozapine therapy. Subsequently, their case notes were reviewed for thromboc Thrombocytopenia was defined as a platelet count of £100 x 109/L (normal range, 150-450 x 109/L).7 The interval between the onset of thrombocytopenia and recovery of platelets to >100 x 109/L was considered as the duration of the thrombocytopenic episode. Patients who had a history of bleeding disorder prior to the initiation of clozapine therapy were excluded. Details about degree, course, clinical manifestations, and complications of thrombocytopenia were noted. Information about age at the time of onset of clozapine therapy, sex, diagnosis, duration of illness, duration of clozapine therapy, concomitant medications, and occurrences of leukopenia, neutropenia, and agranulocytosis were obtained from the case records. In this study, leukopenia was defined as white blood cell count <3 x 109/L (normal range, 4.5-11 x 109/L) and neutropenia and agranulocytosis were defined as absolute neutrophil counts of 0.5-1.5 x 109/L and <0.5 x 109/L (normal range, 1.8-7.8 x 109/L), respectively.4
Statistical Analysis
In view of the small sample size, non-parametric statistical tests, Fisher’s exact test and Mann-Whitney U test, were used to determine group differences. Any finding with p < 0.05 (2-tailed) was considered significant. Computer program SPSS Windows version 7.5 was used for data analysis.
Results
Sociodemographic and Clinical Profiles
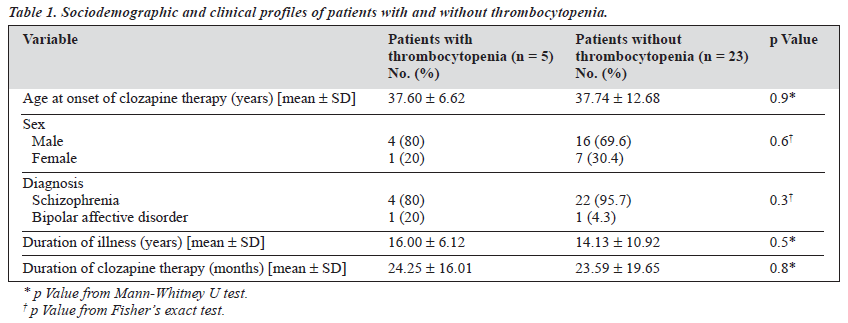
The case records of 380 patients were examined, 28 of whom had received clozapine, and 5 of these (17.8%) had experienced at least 1 episode of thrombocytopenia. All 28 patients who received clozapine were of Indian origin. There was no difference between those who developed thrombocytopenia and those who did not with respect to age at the start of clozapine therapy, sex, psychiatric diagnosis, duration of illness, and duration of clozapine therapy (Table 1).
For clinical reasons involving clozapine-induced side effects, significant mood symptoms, and lack of adequate response, 3 of the 5 patients who had thrombocytopenia were given risperidone (n = 1), sodium valproate (n = 1), or fluoxetine (n = 1) in combination with clozapine. For the same reasons, patients who did not have thrombocytopenia also received risperidone (n = 1), fluoxetine (n = 1), sodium valproate (n = 5), or trihexyphenidyl (n = 7).
Characteristics of Thrombocytopenia
The 5 patients who had thrombocytopenia received clozapine for a range of 21 to 184 weeks. The minimum interval between the start of clozapine therapy and the appearance of thrombocytopenia was 6 weeks and the maximum interval was 44 weeks. Clozapine was discontinued for 2 patients for 6 and 14 weeks due to non-availability. For these 2 patients, the first episode of thrombocytopenia occurred within a fortnight of restarting clozapine. All 5 patients developed thrombocytopenia while taking therapeutic doses of clozapine ranging from 50 to 400 mg/day (Table 2).
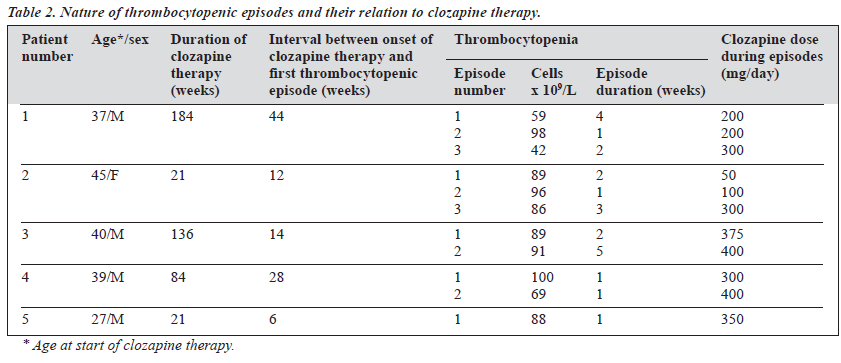
Analysis of the course of thrombocytopenia revealed the following findings. Of 4 patients (80%) who had more than 1 episode of thrombocytopenia, the condition was worse in sub- sequent episodes for 3 patients, (Table 2). The mean interval between the first and second episodes of thrombocytopenia was 8.75 months (standard deviation [SD], 10.30 months; range, 2.00 to 24.00 months). The mean interval between the second and third episodes was 8.50 months (SD, 2.12 months; range, 7.00 to 10.00 months). The episodes of thrombocytopenia lasted for 1 to 12 weeks and all the episodes resolved without reducing the clozapine dosage.
None of the patients had an overt clinical manifestation or complication of thrombocytopenia or other haemato- logical abnormalities such as leukopenia, neutropenia, or agranulocytosis.
Discussion
In this study, 17.8% of patients treated with clozapine developed thrombocytopenia. The rate of thrombocytopenia noted in this study is higher than that of previous reports.4-6 Atkin et al reported patients with platelet counts less than 50 x 109/L only, giving a lower incidence of clozapine- induced thrombocytopenia.4
The results of this study indicate a lack of association between thrombocytopenia and variables such as age at the onset of clozapine therapy, sex, duration of illness, and duration of clozapine therapy. Three of the 5 patients who had thrombocytopenia received fluoxetine, sodium val- proate, or risperidone in combination with clozapine. Pharmacokinetically, fluoxetine,9,10 sodium valproate,9 and risperidone11 are reported to result in marked, minimal, or no elevation of serum clozapine levels, respectively. While there are no data mentioning thrombocytopenia with fluoxetine, there is evidence indicating the occurrence of thrombocytopenia with sodium valproate.12 However, occurrence of blood dyscrasias, including thrombocytopenia, during sodium valproate and clozapine combination therapy is not noted in the literature.13 Similarly, although thrombo- cytopenia has been documented with risperidone therapy,14 except for agranulocytosis,15 no other blood dyscrasias have been recognised with risperidone and clozapine combination therapy.11 Further, since patients with and without thrombocytopenia in our study received fluo- xetine, sodium valproate, and risperidone, and the onset and recovery of thrombocytopenia occurred without alteration in the doses of these medications, thrombo- cytopenia in these patients could not be definitively attributed to these drugs.
In the present study, most of the patients had more than 1 episode of thrombocytopenia and each episode occurred within the therapeutic dose range of clozapine. Notably, the first episode of thrombocytopenia occurred within a year of clozapine therapy in all 5 patients and within the first 4 months for 3 patients. The onset of thrombocytopenia noted in this study agrees with an earlier report by Eranti and Chaturvedi.6 Our finding that severity of thrombocytopenia in most of the patients who had more than 1 episode increased in subsequent episodes is of high clinical relevance. Although a similar phenomenon is unknown in the literature, this finding needs further evaluation to understand the reasons for such progressive decline of platelets. In the present study, the interval between the episodes was found to be nearly equal. This finding suggests that after the first episode, subsequent episodes of thrombocytopenia start occurring at relatively constant intervals.
Clinical features of thrombocytopenia emerge only when platelet counts fall below 50 x 109/L. Platelet counts between 20 and 50 x 109/L and <20 x 109/L result in prolonged post- traumatic and spontaneous bleeding, respectively.7 In our study, no patients had overt clinical manifestations or complications of thrombocytopenia. This is not surprising as only 1 thrombocytopenic episode fell below the 50 x 109/L threshold.
Although clozapine was discontinued in 6 patients who had platelet counts below 50 x 109/L, Atkin et al failed to mention the course of subclinical thrombocytopenia (platelet count, 50-100 x 109/L).4 In our study, most of the thrombocytopenic episodes were in the subclinical range. Resolution of thrombocytopenia that occurred without clozapine dose reduction thus indicates the transient nature of subclinical thrombocytopenia.
Currently, the relationship between thrombocytopenia and other serious haematological abnormalities seems unclear. In earlier reports, occurrences of thrombocytopenia both with5 and without6 agranulocytosis have been reported. Similar to the later observation,6 none of the patients in this study experienced agranulocytosis. This finding hints at the independent nature of clozapine-induced platelet abnormality.
Some of the drug-induced thrombocytopenias are immunologically mediated.7 The finding that thrombo- cytopenia took place within a fortnight of reintroduction of clozapine in 2 patients in this study suggests the possibility of underlying immunological mechanisms.
The main limitations of this pilot study include its smaller sample size and sample bias, notably the exclusive inclusion of inpatients. Also, bleeding time was not monitored. A prospective study with a larger sample size and detailed haematological monitoring is needed to confirm these findings and to evaluate the clinical significance of clozapine-induced thrombocytopenia.
In conclusion, this preliminary investigation indicates that thrombocytopenia is not an unusual adverse effect of clozapine therapy. Although this adverse effect usually manifests as transient episodes with severity in the subclinical range, regular monitoring of platelet counts may be warranted, at least for some patients who may also require another agent that has thrombocytopenic potential.
Reference
- Wahlbech K, Cheine M, Essali A, Adams C. Evidence of clozapine’s effectiveness in schizophrenia: a systematic review and meta-analysis of randomized trials. Am J Psychiatry 1999;156:990-999.
- Frye MA, Ketter TA, Altshuler LL, et al. Clozapine in bipolar disorder: treatment implications for other atypical antipsychotics. J Affect Disord 1998;48:91-104.
- Young CR, Bowers MB, Mazure CM. Management of the adverse effects of clozapine. Schizophr Bull 1998;24:381-390.
- Atkin K, Kendall F, Gould D, Freeman H, Licherman J, O’Sullivan. Neutropenia and agranulocytosis in patients receiving clozapine in the UK and Ireland. Br J Psychiatry 1996;169:483-488.
- Rudolf J, Grond M, Neveling M, Heiss WD. Clozapine induced agranulocytosis and thrombocytopenia in a patient with dopaminergic psychosis. J Neural Trans 1997;104:1305-1311.
- Eranti S, Chaturvedi SK. Marked thrombocytopenia count variations with- out agranulocytosis due to clozapine. Indian J Psychiatry 1998;40:300-302.
- Kumar V, Cotran RS, Robbins SL. Basic pathology. 6th ed. Philadelphia: WB Saunders Company; 1997.
- World Health Organization. The ICD-10 mental and behavioral disorders: clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992.
- Centorrino F, Baldessarini RJ, Kando JC, et al. Serum concentrations of clozapine and its major metabolites: effects of cotreatment with fluoxetine or valproate. Am J Psychiatry 1994;151:123-125.
- Spina E, Avenoso A, Facciola G, et al. Effect of fluoxetine on the plasma concentrations of clozapine and its major metabolites in patients with schizophrenia. Int Clin Psychopharm 1998;13:141-145.
- De Groot IW, Heck AH, Van Harten PN. Addition of risperidone to clozapine therapy in chronically psychotic patients. J Clin Psychiatry 2001;62:129-130.
- Loiseau P. Sodium valproate induced platelets dysfunction and bleeding. Epilepsia 1981;22:141-146.
- Kando JC, Tohen M, Castillo J, Centorrrino F. Concurrent use of clozapine and valproate in affective and psychotic disorders. J Clin Psychiatry 1994;55:255-257.
- Assian HJ, Kolbinger HM, Rao ML, Laux G. Lymphocytopenia and thrombocytopenia during treatment with risperidone or clozapine. Pharmacopsychiatry 1996;29:227-228.
- Godlesky LS, Sernyak MJ. Agranulocytosis after addition of risperidone to clozapine treatment. Am J Psychiatry 1996;153:735-736.