
East Asian Arch Psychiatry 2016;26:3-9
ORIGINAL ARTICLE 
Dr Andrew Found, PhD, University of Saint Joseph, Macao, PR China.
Address for correspondence: Dr Andrew Found, University of Saint Joseph, Rua de Londres, 16, NAPE, Macao, China. Tel: (853) 8796 4418; Email: andrew_found@usj.edu.mo
Submitted: 22 June 2015; Accepted: 19 October 2015
Objective: A wide range of factors can influence help-seeking attitudes when individuals experience a mental disorder. The current study investigated the relationship between traditional Chinese beliefs related to the aetiology of mental disorders and help-seeking attitudes among elderly participants in Macao.
Methods: In order to ensure the suitability of participants for inclusion in this study, the participants were required to complete an initial screening test using the Short Portable Mental Status Questionnaire (SPMSQ). Participants who successfully passed the test (n = 183) completed a questionnaire that included the Inventory of Attitudes Toward Seeking Mental Health Services (IASMHS), a set of 9 items related to traditional Chinese beliefs about aetiology of mental disorders and demographic items.
Results: The IASMHS scores were higher for female participants and for participants who had completed high school compared with those who had never attended school or who had only completed primary education. Endorsement of traditional Chinese beliefs about the aetiology of mental disorders was higher for male participants. There was a negative correlation between traditional Chinese aetiology beliefs related to mental disorders and help-seeking attitudes.
Conclusion: Traditional Chinese beliefs related to the aetiology of mental disorders are a negative factor that inhibits help seeking. Implications for efforts to increase the utilisation of mental health services by the elderly are discussed.
Key words: Aged; Asian continental ancestry group; Help-seeking behavior; Mental disorders / etiology
At the end of 2014, those aged ≥ 65 years accounted for 8.4% of the Macao population and this is projected to reach 19% by the end of 2031.1 In Hong Kong, the 2011 Population Census reported that 13.3% of the population were aged ≥ 65 years, projected to reach 26.5% by the end of 2031.2,3 As the elderly population increases, so will their health care needs, including mental health. In addition to dementia, the elderly can also experience a range of other mental health issues, including depression, anxiety disorders, and psychosis.4-6
In order to effectively treat mental disorders in the elderly, it is important that help is sought from professional mental health services.7,8 Despite the effectiveness of treatment, underutilisation of mental health services is common and professional services may only be considered after other sources of informal support have failed.9,10 For example, in Australia, less than one-third of people who have psychological problems seek help from mental health professionals.11 Similarly, in Europe, only about a quarter of those with mental disorders seek help from professional mental health services.12
A wide range of inhibitory factors have been identified that reduce help seeking for mental disorders.13,14 In addition, several demographic factors, such as gender and age, have been reported to influence help seeking for mental disorders. In terms of gender, several studies have indicated that women are more likely than men to seek professional help.15-17 Interestingly, some research with Asian participants has not reported a gender difference in help seeking for mental disorders. Masuda et al18 compared college students in the US and Japan and reported significant gender differences in help seeking only for the US college students, but not Japanese college students. Similarly, Atkinson and Gim19 reported no significant overall gender difference in help seeking among Asian-American undergraduate students. In terms of age, some studies have reported greater stigma associated with mental disorders and lower help seeking among the elderly.20-22 Nonetheless as with gender, the results are not consistent and some studies have reported that help seeking is unrelated to age.23,24
In addition to possible gender and age differences, several studies indicate that culture influences help seeking25-27 and underutilisation of mental health services.28 Furthermore, several studies provide evidence that lay beliefs about the causes of mental disorders also influence the likelihood of seeking help and satisfaction with treatment.29,30 Kim and Omizo,31 in a study of Asian American college students, reported that participants who adhered to traditional Asian cultural values reported lower help-seeking intentions. Similarly, Wong and Li,32 in a study in Shanghai, reported that participants with stronger endorsement of traditional Chinese beliefs were less inclined to seek professional help.
Found and Duarte33 investigated the relationship between beliefs about the causes of mental disorders and attitudes towards mental illness. In particular, the extent to which the endorsement of traditional Chinese aetiology beliefs (TCEB) about mental disorders was related to attitudes towards mental illness. The questionnaire included 7 statements related to TCEB about mental disorders. These included fate (e.g. ‘people who suffer from a mental disorder are a victim of fate’), ghosts (e.g. ‘ghosts can cause a mental disorder’), karma (‘a mental disorder can be punishment for bad deeds’), and Fung Shui (‘poor Fung Shui can cause a mental disorder’). Participants were asked to indicate to what extent they agreed with these statements. The results revealed a positive correlation between the endorsement of TCEB and social distance from individuals with a mental disorder. This was taken as indicative of more negative attitudes towards mental disorders for participants with greater endorsement of TCEB. Whether this means that such individuals are also less likely to seek help for a mental disorder is not known.
The present study investigated the relationship between TCEB and help seeking for a mental disorder. Since Found and Duarte33 reported that greater endorsement of TCEB was correlated with more negative attitudes towards mental disorders, it is predicted that, as the endorsement of TCEB increases, the likelihood of help seeking will decrease. The present study was conducted in an elderly population (the vast majority being ≥ 65 years) that previous research has indicated tends to more strongly endorse traditional beliefs and practices in relation to health in general.34-36 To ensure that participants were suitable to take part in the present study, a screening test of cognitive functioning (The Short Portable Mental Status Questionnaire [SPMSQ]) was performed prior to administering the main survey.
Participants
Purposive sampling was used in this study to recruit Macao citizens of Chinese ethnicity aged ≥ 60 years. Participants were recruited from 1 of 5 service centres that are available to all elderly citizens in Macao and that provide general social activities and support for the elderly. Inclusion criteria for participants in the present study were: (a) Macao citizens of Chinese ethnicity; (b) Chinese as a first language; and (c) age ≥ 60 years. Participants were excluded if they had a score of < 8 on the SPMSQ test.
Instruments
The SPMSQ was used as a screening test to select elderly participants who were suitable for inclusion in this study.37 The test consists of 10 questions (e.g. “How old are you?”) with each correct answer scoring 1. Low scores indicate cognitive impairment. If a participant scored < 8 they were excluded from the study. The test-retest reliability of the SPMSQ after 4 weeks is 0.83.37 The SPMSQ has been shown to be a valid screening test for dementia38 producing similar results to the Mental Status Questionnaire.39 In the present study, the Chinese version of the SPMSQ was used and has been shown to be a valid40 and reliable measure in several studies of elderly participants in Hong Kong.41,42 For the present study, the wording of 2 items on the SPMSQ was slightly adjusted to localise the measure for Macao (item 7 was changed to ‘Who is the current Chief Executive?’ and item 8 to ‘Who was the Chief Executive before him?’).
The Inventory of Attitudes Toward Seeking Mental Health Services (IASMHS) is a 24-item questionnaire that is based on Fischer and Turner’s Attitudes Toward Seeking Professional Psychological Help Scale (ATSPPHS).43,44 The IASMHS measures attitudes towards mental health help seeking and includes items such as “If I were to experience psychological problems, I could get professional help if I wanted to”. Responses were measured on a 5-point Likert scale (0 = disagree to 4 = agree). There are 3 subscales in the IASMHS that measure psychological openness, help- seeking propensity, and indifference to stigma. Although these 3 subscales represent different components of help seeking, when summed a total scale score gives an overall measure of help-seeking intention (with higher scores indicating greater intention to seek help). Previous research has reported reliability (Cronbach’s alpha) for the IASMHS as 0.87.45 The validity of the IASMHS as a measure of help-seeking intention has been demonstrated with the IASMHS able to differentiate between participants who had previously used mental health services and those who had not, and also to discriminate between participants with intentions to seek professional and non-professional help.43
Atkinson46 translated the IASMHS into Chinese and reported the reliability (Cronbach’s alpha) in a Chinese sample as 0.70 for the total scale. Ng47 adjusted the Chinese version of Atkinson after taking into consideration Taiwanese culture and language. Cronbach’s alpha for the Chinese sample in Ng’s study was 0.71.47 Similarly, in a sample of college students in Taiwan, the reliability of the IASMHS was reported as 0.72.48 In the present study, the overall reliability of the IASMHS was 0.77.
The questionnaire included 9 items designed to measure the extent to which participants endorsed TCEB for mental disorders. Seven of the items in this measure of TCEB were the same as those used by Found and Duarte.33 The remaining 2 items were created for this study (“Loss of balance or harmony within the body [such as a yin and yang imbalance] can lead to a mental disorder” and “Some people’s mental disorder may be due to their parents’ bad deeds”). These 2 statements were included to enhance the measure’s coverage of the domain of TCEB.49 For each of the items, participants were requested to indicate their level of agreement with the statement on a 6-point Likert-type scale (1 = ‘strongly disagree’, 2 = ‘disagree’, 3 = ‘slightly disagree’, 4 = ‘slightly agree’, 5 = ‘agree’, 6 = ‘strongly agree’). Scores on this scale could range from 9 to 54, with higher scores indicating greater endorsement of TCEB for mental disorders. The reliability of the TCEB measure was 0.74, indicating that it was reliable.
Procedure
Initial consent for this survey was obtained from the directors of the 5 social service centres for the elderly in Macao where participants were recruited. Participants were first asked to complete a consent form that explained the purpose of the survey and to record their agreement to participate in the survey. Participants then completed the SPMSQ. If participants did not achieve a score of ≥ 8 on the SPMSQ, they were not invited to complete the rest of the questionnaire. The remainder of the questionnaire comprised a number of demographic items (including age, gender, highest education level completed, and religious beliefs) followed by 2 instruments (IASMHS and TCEB, in that order). Three research assistants (all registered nurses in Macao) collected data from the participants in a face-to- face interview, providing assistance and answering queries whenever necessary. The amount of assistance required varied. Some participants required relatively less assistance, while other participants had nearly the entire questionnaire read aloud for them.
All information, instructions, questions, and statements were written in traditional Chinese. When available, existing Chinese versions of instruments were used (for the SPMSQ and IASMHS). The remaining materials (consent form, demographic items, and TCEB) were translated into Chinese using a back-translation procedure. The research was conducted in accordance with the ethical procedures of the University of Saint Joseph, Macao.
Data Analysis
Data analysis was performed using IBM’s SPSS version 20. The reliability of each instrument (except the SPMSQ) was computed and mean scores for participants were compared for various demographic factors (e.g. gender, age) using analysis of variance (ANOVA) and post-hoc Tukey and LSD tests when necessary. The correlation between scores on the 2 instruments was calculated.
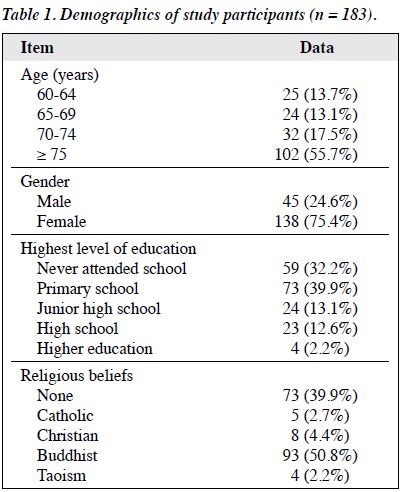
Of a total of 203 participants, 20 were excluded from further investigation based on their score on the SPMSQ. Therefore, data from a total of 183 participants were included in the data analysis, of whom 45 (24.6%) were male and 138 (75.4%) were female and most were aged ≥ 75 years (Table 1). The larger percentage of females was indicative of the fact that more females than males attended the centres for the elderly where the data were collected. Although some participants were aged < 65 years, the vast majority (86.3%) were ≥ 65 years. Generally speaking, the education level of participants was low, with less than 15% having completed high school. In terms of religious beliefs, just over half indicated a Buddhist faith, with other faiths making up less than 10% of the sample. The remaining participants (nearly 40%) did not consider themselves to hold religious beliefs.
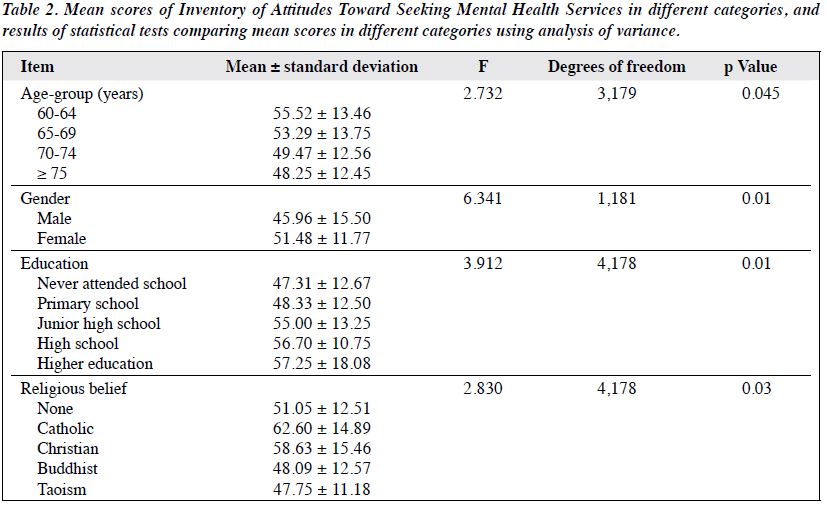
To explore differences based on demographics, scores on instruments in the present study were compared to identify differences related to age, gender, highest education level completed, and religious beliefs. Table 2 shows mean IASMHS scores (measuring help seeking) for different categories for each of these demographic factors. Differences were tested for their statistical significance using one-way ANOVA. The results of these tests indicate that IASMHS scores were significantly different for different age categories. A post-hoc Tukey test did not indicate a significant difference between any of the age categories. Nonetheless a post-hoc LSD test indicated a significant difference in scores between age-groups of 60 to 64 years and ≥ 75 years only (p < 0.05). For gender, IASMHS scores were significantly higher in female participants. Differences in scores were also noted in participants with different education levels. A post-hoc Tukey test indicated that scores were significantly higher for participants who had completed high school compared with those who had never attended school or who had only completed primary school education (both p < 0.05). Finally, in terms of religious beliefs, differences in IASMHS scores were also evident. However, since the number of participants was very low, except in 2 categories of religious belief (none and Buddhist), post-hoc tests were not appropriate. Instead, a t test comparing participants in these 2 categories was performed but did not indicate a significant difference (t = 1.513, degrees of freedom = 164, p = 0.13).
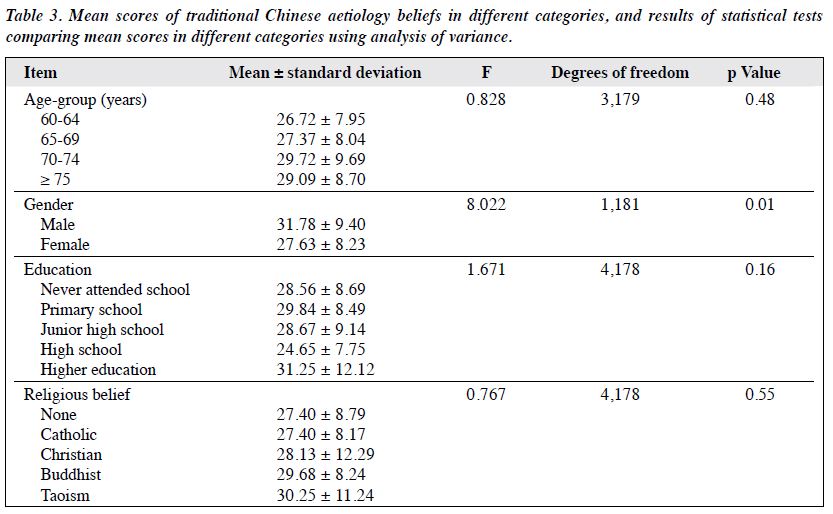
A similar analysis of TCEB scores was conducted for each of the 4 demographic factors — age, gender, highest education level completed, and religious beliefs. As Table 3 shows, the only difference in TCEB scores was related to gender, with a significantly higher mean score for male participants.
Finally, the relationship between TCEB and IASMHS (help seeking) scores was explored using (linear) correlation. This revealed a significant negative correlation between TCEB and IASMHS scores with a correlation coefficient of -0.421 (p < 0.001). In other words, as TCEB scores increased, IASMHS (help seeking) scores decreased.
Estimates of the internal consistency (Cronbach’s alpha) of the 2 measures used in this study, the IASMHS and TCEB, indicated they were adequately reliable measures for the purposes of analysis. The reliability of the TCEB measure was 0.74, and is adequate for a short measure comprising only 9 items.50 For the IASMHS, the reliability in the present study was acceptable at 0.77, though this is lower than that reported for this measure in other studies in Canada and the UK.45,51 Nonetheless, the reliability reported in other studies with Chinese participants has also been lower for the IASMHS compared with participants in the West.46-48 This would suggest that the lower reliability of the IASMHS in the present study is a reflection of cultural differences rather than being due to the sample of participants. Since the IASMHS contains several items that relate to shame and social perceptions (e.g. “I would feel uneasy going to a professional because of what some people would think”), it is possible that these may be interpreted differently within a Chinese cultural context. This may have contributed to the lower reliability reported for the IASMHS in the present study, and other studies with Chinese participants, compared with findings with participants in western countries.
The present study indicated differences in relation to gender, for both help seeking and the endorsement of TCEB. Help seeking (IASMHS) scores were higher for females, indicative of a greater willingness to seek help for a mental disorder. This result is consistent with the results of several studies.15-17 Nonetheless, some research has not reported a gender difference in help seeking. For example, the study of Masuda et al18 compared responses on the ATSPPHS of college students in Japan and the US. The results revealed a significant interaction between nationality and gender, with US females reporting higher scores than US males, and both Japanese males and females. There was no significant difference between the mean scores for male and female Japanese participants. However, the sample in Masuda et al’s study18 was college students, so educational background may have influenced results, perhaps masking differences that may be present in the wider population or an elderly population (as in the present study). The gender difference in help seeking in the present study matches the overall pattern of gender differences reported by other studies, with females reporting greater help-seeking attitudes for mental disorders.
For TCEB scores, male participants reported higher scores, indicative of a greater endorsement of TCEB in relation to mental disorders. Since education level was identified as an important factor influencing TCEB in this study, the gender difference in TCEB scores in the present study could be related to differences in educational achievement between the genders. Despite this, examination of differences in highest education level by gender in the present study did not suggest lower levels of educational achievement for the male participants. Unfortunately, as the percentage of males in the present study was small (n = 45), the number of males in some education levels was very small and precluded meaningful statistical analysis. For participants who had never attended school (n = 59), only 6 were male. Therefore, it seems unlikely that the higher TCEB scores for males can be explained in terms of differences in education level between male and female participants. Instead, for some reason that is unclear from the present data, males tend to more strongly endorse TCEB. Further research is needed to confirm gender differences in the endorsement of TCEB with a larger cross-sectional sample of the population across different age ranges.
As stated in the introduction, the elderly may, in addition to dementia, experience a wide range of mental disorders. As for other age-groups, it is beneficial for professional help to be sought if a mental disorder is experienced. As predicted, the results of the present study reveal that endorsement of TCEB is an additional ‘inhibitory’ factor that can deter individuals from help seeking.14 Research by Kim52 on Asian American college students supports the view of traditional Asian beliefs as inhibitory in relation to help seeking. Kim52 related scores on the Asian Values Scale (AVS), a measure of enculturation to Asian values, with scores for a measure of help seeking (short form of ATSPPHS [ATSPPH-SF]). A hierarchical multiple regression showed that AVS scores were a negative predictor of help seeking (ATSPPH-SF scores), indicating that adherence to (traditional) Asian cultural values was inversely related to help seeking. This finding is consistent with the findings of the present study that showed a negative correlation between TCEB for mental disorders and help- seeking attitudes.
Why might TCEB act as an inhibitory factor in relation to help seeking for a mental disorder? It seems most likely that TCEB influence other factors that are related to the avoidance of help seeking. For example, it is known that stigma is an important inhibitory factor in relation to help seeking.13 One possibility is that individuals who more strongly endorse TCEB may view mental illness and seeking help for a mental illness as more stigmatising, therefore, they report lower levels of help-seeking intention. According to Lam et al,26 traditional Chinese cultural beliefs are rooted in Taoism and Confucianism and Buddhism. As such, “Chinese lay understandings on mental illness tend to be moralising, blaming the individual for the illness”. Within this context, traditional Chinese beliefs concerning mental illness would promote higher levels of stigma in relation to mental illness, and so will act as an inhibitory factor that decreases help-seeking intentions. This is consistent with the results in the present study; as the endorsement of TCEB increased, the help-seeking intentions decreased.
As in the present study, Chen and Mak29 also reported that cultural beliefs about the aetiology of mental disorders influenced help seeking. They suggested that mental health professionals should enhance their awareness of their clients’ beliefs about mental illness and make “culturally appropriate adjustments in the counselling session”. The results of the present study suggest that this may be especially important with elderly clients who may be more likely to endorse TCEB, especially if they are male and have a lower educational background. Nonetheless, this is predicated on the fact that they have sought help in the first place. Therefore, to encourage the elderly in Macao, and elsewhere, to seek professional help, welfare organisations should work to change attitudes of the elderly towards seeking help for mental disorders. This is particularly important for individuals who tend to strongly endorse TCEB in relation to mental disorders and who will likely present more resistance to seeking help.
The present study represents an initial exploration of the relationship between TCEB and help seeking and as such, it incorporates several limitations which should be addressed in further research. First, a larger sample size would enable a more detailed analysis of differences in help-seeking attitudes and the endorsement of TCEB with respect to different demographic variables. Second, the sample in the present study may not be representative of the elderly population in general due to the purposive sampling method adopted. Clearly, elderly Macao citizens who did not attend 1 of the 5 service centres in Macao were not included in the present study and their attitudes may differ from the individuals who do attend a service centre. This is supported by the larger percentage of females in the present study and suggests that the attitudes of some males within the community may not be represented in the present results. Further research is needed to confirm and develop the results of the present study.
Thanks to Mr Nick Ka-Lok Wong for assistance in collecting data for this study.
- Macao population projection. Year 2011-2036. Macao Statistics and Census Service website: http://www.dsec.gov.mo/. Accessed 11 Jun 2005.
- 2011 Population Census summary results. Hong Kong SAR Government Census and Statistics Department website: http://www.census2011.gov.hk/pdf/summary-results.pdf. Accessed 11 Jun 2005.
- Hong Kong SAR Government Census and Statistics Department. Projected mid-year population by age group and sex, February 2015. Census and Statistics Department website: http://www.censtatd.gov.hk/hkstat/sub/sp190.jsp?productCode=D5320182. Accessed 11 Jun 2005.
- Copeland JR, Dewey ME, Wood N, Searle R, Davidson IA, McWilliam C. Range of mental illness among the elderly in the community. Prevalence in Liverpool using the GMS-AGECAT package. Br J Psychiatry 1987;150:815-23.
- Trollor JN, Anderson TM, Sachdev PS, Brodaty H, Andrews G. Prevalence of mental disorders in the elderly: the Australian National Mental Health and Well-Being Survey. Am J Geriatr Psychiatry 2007;15:455-66.
- Howard R, Rabins PV, Seeman MV, Jeste DV. Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: an international consensus. The International Late-Onset Schizophrenia Group. Am J Psychiatry 2000;157:172-8.
- de Jonge P, Huyse FJ, Ruinemans GM, Stiefel FC, Lyons JS, Slaets JP. Timing of psychiatric consultations: the impact of social vulnerability and level of psychiatric dysfunction. Psychosomatics 2000;41:505-11.
- Cuijpers P, van Straten A, Smit F. Psychological treatment of late- life depression: a meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry 2006;21:1139-49.
- Angermeyer MC, Matschinger H, Riedel-Heller SG. What to do about mental disorder — help-seeking recommendations of the lay public. Acta Psychiatr Scand 2001;103:220-5.
- Chen J. Seeking help for psychological distress in urban China. J Community Psychol 2012;40:319-41.
- Andrews G, Issakidis C, Carter G. Shortfall in mental health service utilisation. Br J Psychiatry 2001;179:417-25.
- Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, et al. Use of mental health services in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl 2004;(420):47-54.
- Corrigan P. How stigma interferes with mental health care. Am Psychol 2004;59:614-25.
- Vogel DL, Wester SR, Larson LM. Avoidance of counseling: psychological factors that inhibit seeking help. J Couns Dev 2007;85:410-22.
- Padesky CA, Hammen CL. Sex differences in depressive symptom expression and help-seeking among college students. Sex Roles 1981;7:309-20.
- McKay JR, Rutherford MJ, Cacciola JS, Kabasakalian-McKay R, Alterman AI. Gender differences in the relapse experiences of cocaine patients. J Nerv Ment Dis 1996;184:616-22.
- Addis ME, Mahalik JR. Men, masculinity, and the contexts of help seeking. Am Psychol 2003;58:5-14.
- Masuda A, Suzumura K, Beauchamp KL, Howells GN, Clay C. United States and Japanese college students’ attitudes toward seeking professional psychological help. Int J Psychol 2005;40:303-13.
- Atkinson DR, Gim RH. Asian-American cultural identity and attitudes toward mental health services. J Couns Psychol 1989;36:209-12.
- Griffiths KM, Christensen H, Jorm AF. Predictors of depression stigma. BMC Psychiatry 2008;8:25.
- Roeloffs C, Sherbourne C, Unützer J, Fink A, Tang L, Wells KB. Stigma and depression among primary care patients. Gen Hosp Psychiatry 2003;25:311-5.
- Robb C, Haley WE, Becker MA, Polivka LA, Chwa HJ. Attitudes towards mental health care in younger and older adults: similarities and differences. Aging Ment Health 2003;7:142-52.
- Mackenzie CS, Scott T, Mather A, Sareen J. Older adults’ help-seeking attitudes and treatment beliefs concerning mental health problems. Am J Geriatr Psychiatry 2008;16:1010-9.
- Segal DL, Coolidge FL, Mincic MS, O’Riley A. Beliefs about mental illness and willingness to seek help: a cross-sectional study. Aging Ment Health 2005;9:363-7.
- Haslam N. Dimensions of folk psychiatry. Rev Gen Psychol 2005;9:35- 47.
- Lam CS, Tsang, HW, Corrigan PW, Lee YT, Angell B, Shi K, et al. Chinese lay theory and mental illness stigma: implications for research and practices. J Rehabil 2010;76:35-40.
- Chan B, Ritchie J. Perceptions of Chinese Australians on seeking help for mental health problems: a qualitative study. Int J Ment Health Promot 2011;13:36-45.
- Chen AW, Kazanjian A, Wong H. Why do Chinese Canadians not consult mental health services: health status, language or culture? Transcult Psychiatry 2009;46:623-41.
- Chen SX, Mak WW. Seeking professional help: Etiology beliefs about mental illness across cultures. J Couns Psychol 2008;55:442-50.
- Callan A, Littlewood R. Patient satisfaction: ethnic origin or explanatory model? Int J Soc Psychiatry 1998;44:1-11.
- Kim BS, Omizo MM. Asian cultural values, attitudes toward seeking professional psychological help, and willingness to see a counselor. Couns Psychol 2003;31:343-61.
- Wong DF, Li JC. Cultural influence on Shanghai Chinese people’s help-seeking for mental health problems: implications for social work practice. Br J Soc Work 2012;10:1-18.
- Found A, Duarte C. The etiology of mental disorders: public endorsement of traditional Chinese beliefs in Macau. Int J Soc Psychiatry 2013;59:789-800.
- Rochelle TL, Marks DF. Health behaviors and use of traditional Chinese medicine among the British Chinese. J Cross Cult Psychol 2011;42:390-405.
- Chan MF, Mok E, Wong YS, Tong TF, Day MC, Tang CK, et al. Attitudes of Hong Kong Chinese to traditional Chinese medicine and Western medicine: survey and cluster analysis. Complement Ther Med 2003;11:103-9.
- Chung V, Wong E, Woo J, Lo SV, Griffiths S. Use of traditional Chinese medicine in the Hong Kong Special Administrative Region of China. J Altern Complement Med 2007;13:361-7.
- Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J Am Geriatr Soc 1975;23:433-41.
- Erkinjuntti T, Sulkava R, Wikström J, Autio L. Short Portable Mental Status Questionnaire as a screening test for dementia and delirium among the elderly. J Am Geriatr Soc 1987;35:412-6.
- Hooijer C, Dinkgreve M, Jonker C, Lindeboom J, Kay DW. Short screening tests for dementia in the elderly population. I. A comparison between AMTS, MMSE, MSQ and SPMSQ. Int J Geriat Psychiatry 1992;7:559-71.
- Chi I, Boey KW. Hong Kong validation of measuring instruments of mental health status of the elderly. Clin Gerontol 1993;13:35-51.
- Chi I, Chou KL. Depression predicts cognitive decline in Hong Kong Chinese older adults. Aging Ment Health 2000;4:148-57.
- Chi I, Yip PS, Chiu HF, Chou KL, Chan KS, Kwan CW, et al. Prevalence of depression and its correlates in Hong Kong’s Chinese older adults. Am J Geriatr Psychiatry 2005;13:409-16.
- Mackenzie CS, Knox VJ, Gekoski WL, Macaulay HL. An adaptation and extension of the attitudes toward seeking professional psychological help scale. J Appl Soc Psychol 2004;34:2410-33.
- Fischer EH, Turner JL. Orientations to seeking professional help: development and research utility of an attitude scale. J Consult Clin Psychol 1970;35:79-90.
- Mackenzie CS, Gekoski WL, Knox VJ. Age, gender, and the underutilization of mental health services: the influence of help- seeking attitudes. Aging Ment Health 2006;10:574-82.
- Atkinson NW. Chinese and North American college students’ attitudes toward seeking professional psychological help: gender and ethnic comparisons [thesis]. Humboldt State University, Arcata [CA], US; 2007.
- Ng TS. The level of crisis, attribution and help-seeking attitude in college freshman [thesis]. National Chengchi University, Taiwan; 2009.
- Loo JM, Oei TP, Raylu N. Problem gambling, gambling correlates, and help-seeking attitudes in a Chinese sample: an empirical evaluation. Psychology 2011;2:342-54.
- Mathews M. Assessment and comparison of culturally based explanations for mental disorder among Singaporean Chinese youth. Int J Soc Psychiatry 2011;57:3-17.
- Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ 2011;2:53-5.
- Hyland P, Boduszek D, Dhingra K, Shevlin M, Maguire R, Morely K. A test of the inventory of attitudes toward seeking mental health services. Br J Guid Counc 2015;43:397-412.
- Kim BS. Adherence to Asian and European American cultural values and attitudes toward seeking professional psychological help among Asian American College students. J Couns Psychol 2007;54:474-80.
