
East Asian Arch Psychiatry 2016;26:18-21
ORIGINAL ARTICLE
Mr Chung-Lung Kong, MSc, Kwai Chung Hospital, Hong Kong SAR, PR China. Dr Chi-Chiu Lee, MRCP, FRCPsych , Kwai Chung Hospital, Hong Kong SAR, PR China.
Mr Yee-Chiu Ip, PD (OT), PD (Occupational Safety and Health), Kwai Chung Hospital, Hong Kong SAR, PR China.
Ms Lai-Ping Chow, MBA, BSc, Kwai Chung Hospital, Hong Kong SAR, PR China.
Mr Chi-Hoi Leung, MSc, BNurs, Kwai Chung Hospital, Hong Kong SAR, PR China.
Mr Yiu-Chau Lam, BSc, Kwai Chung Hospital, Hong Kong SAR, PR China.
Address for correspondence: Mr Chung-Lung Kong, Kwai Chung Hospital, 3-15 Kwai Chung Hospital Road, New Territories, Hong Kong SAR, PR China.
Tel: (852) 2959 8148; Fax: (852) 2195 4011; Email: kongcl@ha.org.hk
Submitted: 21 August 2015; Accepted: 24 December 2015
Abstract
Objective: The World Health Organization Five Well-Being Index (WHO-5) has been developed to measure psychological wellbeing. Translation and linguistic validation of the WHO-5 into a Cantonese version has been accomplished for local use but it is not yet validated in people with severe mental illness in Hong Kong. This study aimed to examine the applicability of WHO-5 in measuring the psychological wellbeing dimension of people with severe mental illness. A brief and easily administrated tool to measure psychological wellbeing of people with severe mental illness can be used to provide an outcome measure in research studies and clinical trials.
Methods: Subjects were randomly recruited from the Extended-Care Patient Intensive Treatment, Early Diversion and Rehabilitation Stepping-Stone Project (EXITERS) and the Rehabilitation Activity Centre (RAC) of Kwai Chung Hospital in Hong Kong. They were invited to complete the abbreviated version of Hong Kong Chinese World Health Organization Quality of Life (WHOQOL-BREF [HK]) and WHO-5 (Cantonese version) separately and concurrent validity was examined.
Results: A total of 84 subjects were recruited, 42 each from EXITERS and RAC. In all, 49 (58%) were male and 35 (42%) were female. The mean ± standard deviation age was 43.2 ± 9.7 years. Their mean duration of mental illness was 16.4 ± 10.5 years and the mean years of education was 10.17 ± 2.5 years, i.e. about junior secondary school level in Hong Kong. The internal consistency of the WHO-5 was satisfactory (0.86) and was comparable with previous reports. Regarding validity, 1-factor structure with an eigenvalue of 3.24 explained 64.8% of total variance of WHO-5 for people with severe mental illness. Concurrent validity was established with moderate correlation (0.41-0.51) between WHO-5 and 4 domains of the WHOQOL-BREF (HK).
Conclusion: The WHO-5 (Cantonese version) is a reliable and valid tool to assess the psychological wellbeing of people with severe mental illness in Hong Kong. It can be used to monitor the effectiveness of psychological intervention aimed at improving the wellbeing of such patients.
Key words: Mental disorders; Mental health; Quality of life
Introduction
Quality of life (QOL) has been defined by the World Health Organization (WHO) as an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns. It is a broad concept and affected in a complex way by sociocultural, health, and psychological wellbeing dimensions.1 It has become an increasingly important concept as an outcome measure in the evaluation of treatment and in many clinical trials that involve people with severe mental illness.2
Mental illness frequently causes impaired functioning in more than one life aspect such as functional performance, as well as social and vocational functioning.3 Affected individuals are also often stigmatised by others and face social isolation, social distance, unemployment, homelessness, and institutionalisation.4 Such experiences are complex and have negative or undesired consequences on the way in which they feel about their lives. Traditionally, objective indicators such as duration of hospitalisation and re-hospitalisation rates are used to determine the quality of services or interventions delivered to people with severe mental illness.5,6 Nonetheless, such indicators do not adequately reflect how they perceive their personal wellbeing as a result of the mental health services received. Thus measurement of QOL or psychological wellbeing serves as essential outcome indicators.
The World Health Organization Five Well- Being Index (WHO-5) has been developed to measure psychological wellbeing.7 Translation into a Cantonese version and linguistic validation of the WHO-5 has been accomplished for local use, but is not yet validated in people with severe mental illness in Hong Kong.
The abbreviated version of Hong Kong Chinese World Health Organization Quality of Life (WHOQOL- BREF [HK]) has been widely used to measure QOL in many mental health studies and service projects in Hong Kong. It has been developed and validated in a way to ensure relevancy to the local culture. It is useful in the assessment of long-term treatment outcome when patients have returned to the community but is too lengthy and inconvenient for use in daily clinical practice.8 The content of the items were not designed for inpatients. Therefore, this study aimed to examine the applicability of WHO-5 in measuring the psychological wellbeing dimension of people with severe mental illness. A brief and easily administrated tool to measure the psychological wellbeing of people with severe mental illness can be used to provide an outcome measure in research studies and clinical trials.
Methods
Subjects
Subjects aged between 18 and 65 years, with a diagnosis of schizophrenia, schizotypal and delusional disorders (F20- F29) according to the ICD-10 were randomly recruited by convenient sampling from the Extended-Care Patient Intensive Treatment, Early Diversion and Rehabilitation Stepping-Stone Project (EXITERS), a purpose- built rehabilitation service for inpatients that bridges inpatient psychiatric care and community living; and the Rehabilitation Activity Centre (RAC), a day hospital of the Community and Rehabilitation team in Kwai Chung Hospital, Hong Kong.
Data Collection
Subjects at EXITERS and RAC who met the selection criteria were invited to participate in this study. A letter of invitation was provided to explain the aim of the study. Those who agreed to participate were requested to provide written consent prior to the study commencement. This was a cross-sectional study, and face-to-face interviews were conducted to solicit information on socio-demographic characteristics. Individuals were then invited to complete the WHOQOL-BREF (HK) and WHO-5 separately. Data were recorded on the General Data Base Form tailor-made for this study.
Instrumentation
General Data Base Form
This form was designed to collect data on the socio- demographic characteristics, and the raw scores of WHOQOL-BREF (HK) and WHO-5 (Cantonese version) of the subjects.
World Health Organization Five Well-Being Index
The WHO-5 was originally derived from a larger rating scale developed for a WHO project on QOL in patients with diabetes. It has been widely used in different settings and translated into many languages (http://www.who-5.org). High reliability, validity, and sensitivity of the WHO-5 has been demonstrated for assessing patient outcome and monitoring patient response to treatment in the psychiatric services.9 According to Henkel et al,10 the administration of WHO-5 is considerably faster than other measures of mental health status without compromising sensitivity or specificity.
The WHO-5 is a short and quick self-administrated tool to measure the psychological wellbeing over the preceding 2 weeks on a 6-point Likert scale graded from 0 (at no time) to 5 (all of the time). Total score ranges from 0 to 25, with a higher score indicating an increased sense of psychological wellbeing.11 It was translated into a Hong Kong Cantonese version through independent forward and backward translation and expert panel review. Linguistic validation was completed to ensure its applicability to local culture. Good internal consistency (Cronbach’s α = 0.86) and test-retest reliability (intraclass correlation coefficient [1,1] = 0.83) were demonstrated in samples of elderly people.12
The Abbreviated Version of Hong Kong Chinese World Health Organization Quality of Life
The WHOQOL-BREF (HK) has been developed and validated in a way to ensure relevancy to the Hong Kong culture. It has been used to assess QOL with good reliability and validity. It comprises 2 national items and 26 items as in the English version of the WHOQOL-BREF (HK) making a 28-item questionnaire that covers 4 domains of QOL, including physical health, psychological, social relationship, and environmental domains.
Statistical Analysis
Data were analysed with the Statistical Package for the Social Sciences Windows version 18.0 (SPSS Inc., Chicago [IL], US). Descriptive statistics were used for analysis of the socio-demographic characteristics and clinical data of the subjects. The reliability of WHO-5 (Cantonese version) was measured through Cronbach’s alpha coefficient, as well as inter-item and item-total correlation coefficients. A value between 0.7 and 0.9 of Cronbach’s alpha coefficient, inter-item correlation coefficients of < 0.80 and > 0, and item-total correlation coefficients of > 0.20 were regarded as satisfactory.13 An item was accepted for removal if its deletion caused a > 0.1 increase in Cronbach’s alpha coefficient.
Exploratory factor analysis was applied to explore the factor structure of WHO-5 (Cantonese version) of the study sample. Dixon14 stated that criteria for retaining factors were an eigenvalue > 1, jointly explaining > 50% of the total variance and factor loadings > 0.40. Principal component analysis was applied as the factor extraction method and the varimax rotation method was chosen for matrix interpretation.
Pearson’s correlation analysis was applied to explore the correlation between the WHOQOL-BREF (HK) score and WHO-5 score (Cantonese version) for concurrent validity. Throughout the study, the significance level was set at p < 0.05.
Ethical Issue
The research study was performed with reference to the principles of the Declaration of Helsinki.15 Ethical approval was granted by the Research Ethics Committee, Kowloon West Cluster, Hospital Authority of Hong Kong.
Results
Subjects
A total of 84 subjects were recruited, 42 each from EXITERS and RAC. In all, 49 (58%) were male and 35 (42%) were female. Their mean (± standard deviation) age was 43.2 ± 9.7 years. The mean duration of mental illness was 16.4 ± 10.5 years and their mean duration of education was 10.17 ± 2.5 years, i.e. about junior secondary school level in Hong Kong.
Reliability of World Health Organization Five Well- Being Index
The Cronbach’s alpha coefficient for WHO-5 (Cantonese version) was 0.86. The inter-item correlation coefficients were between 0.46 and 0.74. All corrected item-total correlation coefficients were between 0.59 and 0.77. All items, if deleted, would result in a slight reduction in Cronbach’s alpha coefficient (0.01-0.05) only.
Validity of World Health Organization Five Well- Being Index
Exploratory Factor Analysis
The Kaiser-Meyer-Olkin measure of sample adequacy was 0.823 and Bartlett’s test of sphericity was X2 = 189.25 (p < 0.001), indicating the suitability of the collected data for factor analysis. Exploratory factor analysis was then conducted and yielded 1 factor with an eigenvalue of 3.24 that explained 64.8% of total variance. Factor loading for all items was > 0.73.
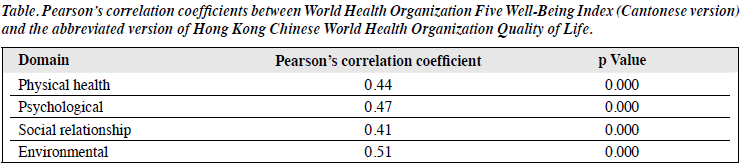
Concurrent Validity
The Pearson’s correlation coefficients between WHO-5 (Cantonese version) and WHOQOL-BREF (HK) are listed in the Table.
Discussion
The present report is the first to evaluate the reliability and validity of the WHO-5 (Cantonese version) for people with severe mental illness. The internal consistency of the WHO-5 was satisfactory (0.86) and was comparable with previous reports, i.e. 0.8516 and 0.87.17 Regarding the validity, 1-factor structure had an eigenvalue of 3.24, which explained 64.8% of total variance of WHO-5 for people with severe mental illness. These results are similar to previous studies where 1-factor structure was reported with total variance of 63.1%16 and 66.8%.17 Concurrent validity was established with moderate correlation (0.41- 0.51) between WHO-5 and 4 domains of WHOQOL-BREF (HK). These findings support the use of WHO-5 as a valid means to monitor the psychological wellbeing of people with severe mental illness.
Limitations
There are limitations to the study. The sample size of the study was relatively small and results cannot be generalised. Nonetheless, the case medical officers had confirmed the suitability of study subjects to join the study although severity of their symptoms was not measured. Therefore, it is suggested that we can control this factor in future study.
Conclusion
There are various outcome measures in mental health and often objective. Subjective indicators such as psychological wellbeing, however, are vital to understand the effectiveness of the recovery-oriented mental health service delivery. The WHO-5 (Cantonese version) is a reliable and valid tool to assess the psychological wellbeing of people with severe mental illness in Hong Kong. It can be used to monitor the effectiveness of psychological interventions aimed at improving the wellbeing of patients with severe mental illness.
References
- de Souza CM, Hidalgo MP. World Health Organization 5-item well- being index: validation of the Brazilian Portuguese version. Eur Arch Psychiatry Clin Neurosci 2012;262:239-44.
- Meijer CJ, Koeter MW, Sprangers MA, Schene AH. Predictors of general quality of life and the mediating role of health related quality of life in patients with schizophrenia. Soc Psychiatry Psychiatr Epidemiol 2009;44:361-8.
- Sadock BT, Sadock VA. Kaplan and Sadock’s comprehensive textbook of psychiatry. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2000.
- World Psychiatric Association. The World Psychiatric Association global programme to reduce the stigma and discrimination because of schizophrenia. Schizophrenia — open the doors training manual. Geneva: World Psychiatric Association; 2005.
- Browne S. Rehabilitation programmes and quality of life in severe mental illness. Int J Soc Psychiatry 1999;45:302-9.
- Korr WS, Ford BC. Measuring quality of life in the mentally ill. Qual Life Res 2003;12 Suppl 1:17-23.
- Bech P. Quality of life in the psychiatric patient. London: Mosby- Wolfe; 1998.
- Ng SS, Lo AW, Leung TK, Chan FS, Wong AT, Lam RW, et al. Translation and validation of the Chinese version of the short Warwick- Edinburgh Mental Well-being Scale for patients with mental illness in Hong Kong. East Asian Arch Psychiatry 2014;24:3-9.
- Newnham EA, Hooke GR, Page AC. Monitoring treatment response and outcomes using the World Health Organization’s Wellbeing Index in psychiatric care. J Affect Disord 2010;122:133-8.
- Henkel V, Mergl R, Kohnen R, Maier W, Möller HJ, Hegerl U. Identifying depression in primary care: a comparison of different methods in a prospective cohort study. BMJ 2003;326:200-1.
- Bech P, Olsen LR, Kjoller M, Rasmussen NK. Measuring well-being rather than the absence of distress symptoms: a comparison of the SF-36 Mental Health subscale and the WHO-Five Well-Being Scale. Int J Methods Psychiatr Res 2003;12:85-91.
- Leung KF, Wong WW. Translation and validation of the WHO (Five) Well Being Index (WHO-5). Hong Kong: Queen Elizabeth Hospital, Pok Oi Social Service; 2005.
- Streiner DL, Norman GR. Health measurement scales: a practical guide to their development and use. U.K.: Oxford University Press; 1995.
- Dixon J. Factor analysis. In: Munro BH, editor. Statistical methods for health care research. 4th ed. Philadelphia, Lippincott; 2001:303-31.
- World Medical Association. Declaration of Helsinki — Ethical principles for medical research involving human subjects. Adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1994, and amended by the 59th WMA General Assembly, Seoul, Korea, October 2008.
- Mortazavi F, Mousavi SA, Chaman R, Khosravi A. Validation of the World Health Organization-5 Well-Being Index; assessment of maternal well-being and its associated factors [in Turkish]. Turk Psikiyatri Derg 2015;26:48-55.
- Saipanish R, Lotrakul M, Sumrithe S. Reliability and validity of the Thai version of the WHO-Five Well-Being Index in primary care patients. Psychiatry Clin Neurosci 2009;63:141-6.
