
East Asian Arch Psychiatry 2011;21:91-98
ORIGINAL ARTICLE
Dr Andrew Found, PhD, University of Saint Joseph, Macao, China.
Dr Carlos Duarte, MD, Macao Psychiatric Hospital, Macao, China.
Address for correspondence: Dr Andrew Found, University of Saint Joseph, Rua de Londres, 16, NAPE, Macao, China.
Tel: (853) 8796 4418; Email: andrew_found@usj.edu.mo
Submitted: 4 January 2011; Accepted: 6 May 2011
Abstract
Objectives: To investigate the effects of different Chinese terms for mental illness and related symptoms on the attitudes of adolescents towards sufferers of a mental illness.
Methods: A survey of 578 secondary school students attending 4 schools in Macao was conducted. Each student read a short passage about a new student with a mental illness joining their class. Different versions used different labels to refer to the illness of the new student. The symptoms describing the new student also varied: either describing positive symptoms of schizophrenia or mild negative symptoms only. The attitudes of participants to the new student described were measured.
Results: There were significantly more negative attitudes towards the sufferer of a mental illness referred to with a psychiatric label, compared with a general label ‘illness’. Participants also expressed significantly more negative attitudes when positive symptoms of schizophrenia were used to describe the new student. The results are discussed in terms of the influence of labels and symptoms on attitudes towards mental illness.
Conclusions: These results supported the existence of 2 additive costs in terms of negative attitudes towards sufferers of mental illness, one associated with the label and the other associated with the symptoms.
Key words: Asian continental ancestry group; Attitude; Mentally ill persons; Social stigma; Stereotyping
摘要
目的:透过形容描述精神病的不同字眼和相关症状,检视青少年对精神病患者的态度。
方法:研究以问卷形式访问来自澳门4间学校的578名中学生。每名学生阅读一篇有关患有精神病的新生的短文,并以形容那位新生病症的不同字眼製作其他短文版本。透过不同的病徵:精神分裂症的正向症状或轻微的负向症状,评估参与者对短文所描述的新生的态度。
结果:结果显示,如果患者的病症被标籤化,相对被称为「普通」患者而言,参与者对前者的态度较为负面;当形容患者有正向症状的时候,参与者的态度也较消极。本文也以病症被标籤化和症状这两项因素,对精神病患者态度的影响作深入讨论。
结论:问卷的结果支持作者的论据:病症被标籤化和症状是对精神病患者持负面态度的2项附加因素。
关键词:亚洲大陆血统群、态度、精神病患者、社会耻辱、定型
Introduction
The Chinese term for mental illness (‘Jing-shen-bin’ [精神病]) and the Chinese term for schizophrenia (‘Jing-shen-fen- lie-zheng’ [精神分裂症]’, literally ‘mind-split disease’), both elicit substantial negative attitudes and contribute to significant levels of stigma.1,2 The stigma associated with these labels and their negative impact in terms of the prognosis of sufferers3 led some mental health professionals to propose a change to the labels used for serious mental disorders, particularly for schizophrenia.4,5 This need may be especially acute in Japanese and Chinese cultures, which use a character-based writing system.6 In both Japan and Hong Kong, the stigmatising effect of traditional labels for schizophrenia was considered sufficiently detrimental that new terms have been introduced and adopted by mental health professionals. In Japan, the term ‘togo-shiccho- sho’ (literally ‘integration disorder’) has been adopted7 and in Hong Kong the term ‘Si-jue-shi-diao’ (‘思覺失調’, literally ‘dysregulation of thought and perception’) is now in use.8 However, it is unclear whether simply changing the descriptive labels used by clinicians to refer to different mental disorders is actually effective in influencing the negative attitudes and concomitant behaviour towards sufferers of mental illness.9
To investigate this question in the context of Hong Kong, the effect of changing the label used to describe schizophrenia on attitudes towards sufferers was explored.10 In their study, attitudes towards different labels for mental illness / psychosis were investigated using questionnaires administered to secondary school students, in particular, whether the newly introduced label for schizophrenia (‘Si-jue-shi-diao’) would elicit less negative attitudes towards sufferers. The present study examined the previous findings10 in Macao. Macao became a special administrative region of China after Portuguese rule ended in 1999 and is approximately 60 kilometres from Hong Kong. As close neighbours, Hong Kong and Macao are similar with respect to language and culture although Macao’s small size, history, and prominent gaming industry also give it a distinct feel.
In Chung and Chan’s study,10 the participants read a short passage (‘vignette’) about a student described as experiencing positive symptoms of schizophrenia. In the study, 4 different versions of the vignette were used which differed in terms of the labels used by a doctor who diagnosed the student in the vignette (either ‘Jing-shen-bin’, ‘Si-jue-shi-diao’, ‘Jing-shen-fen-lie-zheng’, or no label). In addition to these 4 label conditions, the gender of the student in the vignette was varied randomly by using either a male (‘Ka-Hung’) or female name (‘Ka-Yan’). After reading the vignette, the participants in the study indicated their attitudes towards the protagonist by signifying agreement with a series of statements related to the protagonist, from which a measure of social distance was derived. The respondent’s perceived likelihood of interacting socially with the student in the vignette (e.g. ‘I would not invite Ka-Hung to my birthday party’) was indicated on a 4-point Likert scale (‘strongly disagree’, ‘disagree’, ‘agree’ or ‘strongly agree’).
The results of the previous study10 revealed no significant difference in social distance scores for the 4 different label conditions, including when the protagonist in the vignette was labelled with schizophrenia (either ‘Jing-shen-fen-lie-zheng’ or the new term ‘Si-jue-shi-diao’) compared with when no label was specified. These results suggested that different labels do not influence attitudes towards a sufferer from schizophrenia. This result is interesting as it is at odds with the strongly negative attitudes that terms relating to mental illness usually provoke.11,12
However, further examination of the vignette and measurement of social distance suggests other potential explanations as to why respondents did not indicate different attitudes to the different labels.10 Firstly, the protagonist described in the vignette may have lacked personal relevance to the respondent, resulting in relatively neutral attitudes towards them. In addition, the measure of social distance may have worked against the expression of different attitudes in the different label conditions — some of the statements expressed fairly strong attitudes that may have discouraged variation in responses; also, the limited range of response categories afforded by the 4-point Likert scale may have served to ‘compress’ responses.13 The present research aimed to explore these issues by emphasising personal relevance and encouraging a greater range of responses to test whether differences in attitudes towards different labels do become manifest.
To facilitate comparison, the present study was similar and sampled the attitudes of secondary school students to another student described in a vignette. Personal relevance to the respondent was increased by describing a new student that joins the respondent’s class. The vignette then described the behaviour of the new student observed from the perspective of the respondent. The wording of the vignette was designed to make the protagonist personally relevant to the respondent (“A new student joining your class”). The measurement of social distance in the present study was also modified to encourage a greater variation of responses. Firstly, instead of the 4-point scale,10 the present study used a 6-point scale. The aim was to allow for a greater variation in responses. The statements used in the present study to measure social distance were modified to express ‘milder’ attitudes towards the protagonist. For example, the statement in the present study was described as “I would not like to talk to Ka-Hung”. The aim was to encourage the expression of a wider range of responses.
As well as the changes to the vignette and measurement of social distance, the present study also introduced a new variable — symptoms. Another possible reason for not observing a difference in the 4 label conditions was that the symptoms described in the vignette were the same in each, although the label changed.10 It is possible that the symptoms were an overriding determinant of the degree of social distance between the subject of the vignette and the respondent, masking any label-related differences. To explore this possibility, the symptomatology described in the present study was manipulated independently of the label. In half of the vignettes, the protagonist was observed as experiencing the positive symptoms of schizophrenia (delusions and hallucinations). In the other half, the protagonist was observed with only mild negative symptoms of schizophrenia (quiet, withdrawn). The inclusion of a symptomatology variable in the present study allowed the influence on attitudes towards the protagonist to be compared, with respect to the following questions: (1) Do different psychiatric labels, in the absence of positive symptoms, elicit different levels of negative attitudes based on the stigma associated with them? (2) What are the relative contributions of the label and the symptoms on attitudes towards a sufferer from mental illness?
Methods
This survey measured attitudes of secondary school students in Macao towards a new classmate described in a ‘vignette’, which referred to the new classmate by one of several different mental illness–related labels, as follows:
- A general label (the classmate is simply referred to as having an ‘illness’);
- The label refers to ‘Jing-shen-bin’ (mental illness);
- The label refers to ‘Si-jue-shi-diao’ (a newly introduced term to replace ‘Jing-shen-fen-lie-zheng’ in Hong Kong); and
- The label refers to ‘Jing-shen-fen-lie-zheng’ (the term for schizophrenia).
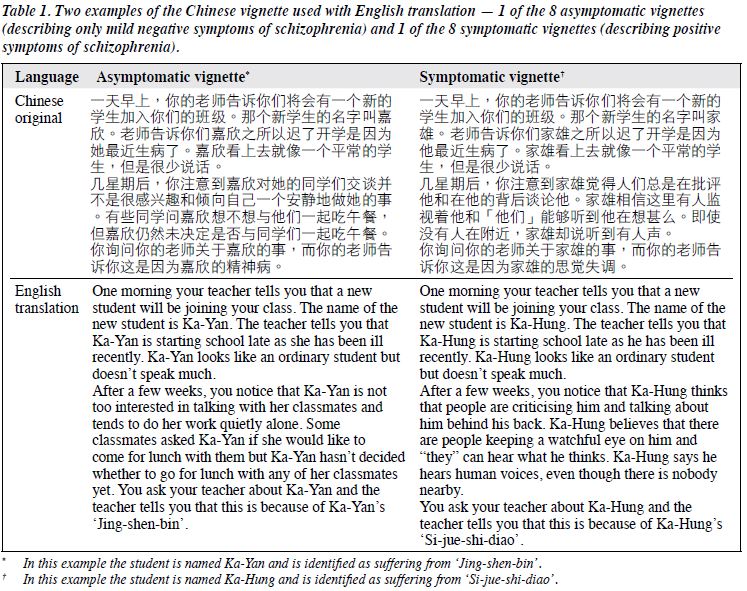
As well as these 4 label conditions, the symptoms displayed by the new classmate were also varied. In half of the questionnaires, the student in the vignette was described as experiencing positive symptoms of schizophrenia (hearing voices, delusions). In the other half of the questionnaires, the student was describing in terms of only mild negative symptoms of schizophrenia (quiet, withdrawn). The gender of the new classmate was varied randomly by using either a male (‘Ka-Hung’) or female (‘Ka-Yan’) name. Therefore, 16 different versions of the same questionnaire were used, that differed in terms of the gender of the new classmate, symptomatology, and the label used to refer to the new classmate’s condition. The appropriate ethical procedures of The University of Saint Joseph and for Macao were adhered to during the research. Two examples of the Chinese vignette used (1 asymptomatic and 1 symptomatic) along with an English translation are shown in Table 1.
Participants
A total of 578 students attending 4 secondary schools in Macao consented to complete the questionnaire. All were co-educational, mainstream schools selected to be representative of the general school population of Macao. Of the 578 respondents who returned the questionnaire, 3 did not indicate either their gender or age and were excluded from the analysis. Among the remaining 575, 290 (50.4%) were female and 285 (49.6%) male. The mean (standard deviation [SD]) age of respondents was 16.7 (1.5) years, ranged from 13 to 20 years. In all, 81 (14%) of the respondents indicated they had religious beliefs: 29 (36%) were Catholic, 16 (20%) were Christian, 29 (36%) were Buddhist, and 7 (8%) had other faiths.
Materials
Each questionnaire was printed on a single sheet of paper. The front side included instructions, demographics, and the ‘vignette’. The reverse side listed the questionnaire items and response categories in a table format. All questionnaires were written in traditional Chinese characters.
Procedures
The questionnaire was administered to a large group of students at the same time (generally one class). To begin with, the questionnaire administrator gave a brief set of instructions to the students explaining that participation was voluntary, anonymous and not related to their school (the teacher was not present). Students were encouraged to give honest answers and not to talk to each other until everyone had completed the questionnaire. The different versions of the questionnaire were handed out randomly. Once all of the students had completed them, they were collected by the administrator.
Measures
The questionnaire consisted of 3 sections. The first dealt with demographics; students were asked to indicate their gender, age, and religious beliefs. The second was the vignette containing the text describing a ‘new student’. The last section measured attitudes towards the new student, in which respondents indicated agreement with 17 statements related to the new student (e.g. “I would not like to talk to Ka-Hung”) on a 6-point Likert scale (‘strongly disagree’, ‘disagree’, ‘slightly disagree’, ‘slightly agree’, ‘agree’, and ‘strongly agree’). Of these, 9 statements measured social distance and were based on the items used by Chung and Chan10; the remaining 8 statements referred to the protagonist of the vignette and related to other attitudes relevant to mental illness (e.g. “Ka-Hung could hurt someone”). A complete list of statements is shown in Table 2.
Statistical Analysis
An exploratory factor analysis was conducted to extract reliable measures of respondent attitudes towards the protagonist in the vignette. These measures were then analysed using a factorial analysis of variance which identified significant differences in measure scores for the factors of label, symptomatology, gender of respondent, and gender of protagonist.
Results
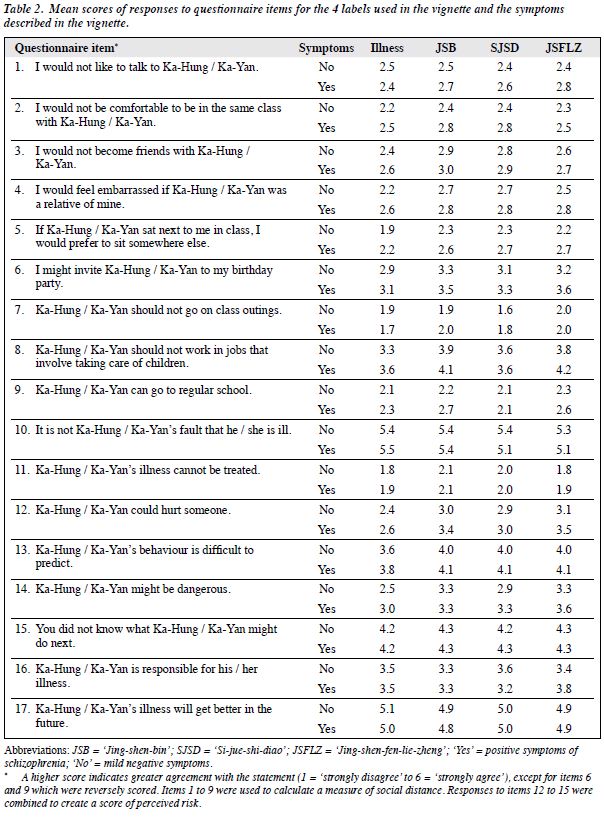
Table 2 shows mean responses to the 17 items for each of the 4 label conditions according to the symptomatology described in the vignette. Responses to the first 9 items, which measured social distance, showed acceptable reliability with a Cronbach’s alpha of 0.81. The total scores for these 9 items were divided by 9 to give a mean social distance score per item for each respondent. The remaining 8 statements were factor analysed (principal component analysis with varimax rotations) which revealed 3 underlying factors (all loadings > 0.4). Items 12 to 15 (Table 2) were closely related to a common factor and were combined to create a measure referred to as perceived risk, which had acceptable reliability with a Cronbach’s alpha of 0.78. The total scores for these 4 items were divided by 4 to give a mean perceived risk score per item for each respondent. The 2 remaining factors both comprised of 2 of the 4 remaining items. However, the low reliability (Cronbach’s alpha of 0.57 and 0.23) of these factors precluded their meaningful analysis.
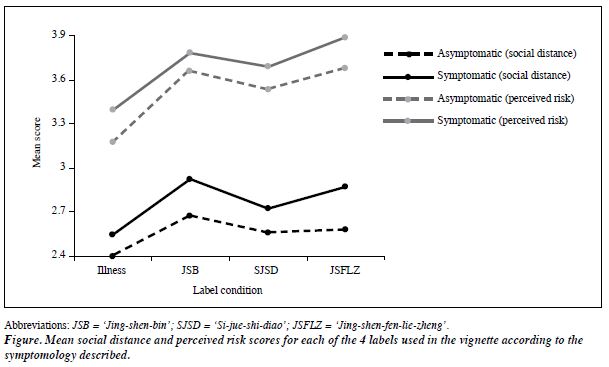
The Figure shows the mean social distance and perceived risk scores for the 4 label conditions according to the symptomatology described in the vignette. The mean (SD) social distance score for all respondents was 2.66 (0.73), while the mean (SD) perceived risk score for all respondents was 3.61 (0.91). The Figure shows a clear difference in both mean social distance and perceived risk scores based on the symptoms described in the vignette. For all 4 labels, scores were higher when the vignette included positive symptoms of schizophrenia. Mean social distance and perceived risk scores for the label ‘illness’ were lower compared with other labels.
To investigate the significance of the differences, an analysis of variance was conducted on social distance scores (with factors related to the label and symptomatology). Both the main effect of label (F3,549 = 5.42, p = 0.001) and symptomatology (F1,549 = 12.42, p < 0.001) were significant whereas the interaction was not significant (F3,549 = 0.30, p = 0.82). A post-hoc Tukey test revealed that social distance scores for the label ‘illness’ were significantly lower than that for the labels ‘Jing-shen-bin’ (p = 0.001) and ‘Jing-shen-fen-lie-zheng’ (p = 0.02), but not significantly different from scores for the label ‘Si-jue-shi-diao’ (p = 0.19).
An analysis of variance on perceived risk scores (with factors of label and symptomatology) confirmed that both the main effect of label (F3,563 = 8.28, p < 0.001) and symptomatology (F1,563 = 5.73, p = 0.02) were significant, whereas the interaction was not significant (F3,563 = 0.10, p = 0.96). A post-hoc Tukey test revealed that perceived risk scores for the label ‘illness’ were significantly lower than that for the labels ‘Jing-shen-bin’ (p < 0.001), ‘Jing- shen-fen-lie-zheng’ (p < 0.001), and ‘Si-jue-shi-diao’ (p = 0.02).
To explore gender influences, an analysis of variance (with factors of the label, symptomatology, gender of the respondent and of the protagonist) was performed on social distance scores. The main effect of respondent’s gender was not significant (F1,525 = 2.63, p = 0.11), whereas that of the protagonist’s gender was significant (F1,525 = 11.50, p = 0.001). The only significant interaction was between the label and gender of the respondent (F3,525 = 3.40, p = 0.02). This was mostly due to lower social distance scores for the label ‘Jing-shen-fen-lie-zheng’ for male compared with female respondents. Four t tests comparing social distance scores of male and female respondents for each of the 4 labels confirmed this, with only scores for the label ‘Jing-shen-fen-lie-zheng’ being significantly lower in male (mean [SD] = 2.54 [0.77]) than female (mean [SD] = 2.94 [0.69]) respondents (t (140) = 3.24; p = 0.001).
The relationship between perceived risk scores and gender of the respondent and protagonist was slightly different to that observed for social distance scores. The mean perceived risk scores for female respondents were higher overall. In contrast, perceived risk scores were lower overall for female protagonists. An analysis of variance (with factors of label, symptomatology, gender of respondent and protagonist) confirmed this pattern. Both the main effects of respondent’s gender (F1,539 = 5.48, p = 0.02) and protagonist’s gender (F1,539 = 4.94, p = 0.03) were significant. The only significant interaction was between the label and gender of the respondent (F3,539 = 3.97, p = 0.01). Four t tests comparing perceived risk scores of male and female respondents for each of the 4 labels also confirmed that this was related to scores for the label ‘Jing-shen-fen- lie-zheng’. Scores for this label were significantly lower for male (mean [SD] = 3.52 [1.05]) than female (4.08 [0.74]) respondents (t (142) = 3.58; p < 0.001).
For the remaining 4 questionnaire items in Table 2, respondents largely disagreed with item 11 (mean [SD] = 1.94 [0.98]), agreed with items 10 (5.33 [1.06]) and 17 (4.93 [0.99]), and were relatively neutral with respect to item 16 (3.44 [1.28]). Overall, respondents indicated optimism that the protagonist could (item 11) and would (item 17) get better in the future, and they were not responsible for their own illness (item 10).
Discussion
The present study found a significant difference in attitudes for different labels. Compared with the general label ‘illness’, more negative attitudes for the labels ‘Jing- shen-bin’ (mental illness) and ‘Jing-shen-fen-lie-zheng’ (schizophrenia) were expressed but not for the label ‘Si-jue- shi-diao’ (psychosis). This result confirms that psychiatric labels are associated with significant stigma, and that introduction of a new term may mitigate this to some degree. The results of the present study also demonstrated the significant influence of symptomatology on attitudes, with more negative attitudes expressed towards the student in the vignette when the positive symptoms of schizophrenia were described, independent of the label used to refer to the student.
Why, despite the similarities between the 2 studies, were different results observed in the present study compared with the one by Chung and Chan?10 The personal relevance of the vignette to the respondent was enhanced; also, the measurement of attitudes towards the protagonist was modified to encourage a greater range of responses. These changes were sufficient to ‘tease out’ significant differences in attitudes towards different labels and demonstrated the important role of symptomatology in influencing attitudes.
In our study, the respondents indicated significantly lower social distance score to the general label ‘illness’, when compared with the traditional psychiatric labels of mental illness and ‘schizophrenia’. The ambiguous nature of the label ‘illness’ presumably meant that some of the respondents may not identify the protagonist as suffering from a mental illness, particularly in the absence of positive symptoms. The Figure, however, shows that even when positive symptoms of schizophrenia were described, social distance scores for ‘illness’ were still lower than that for a specific psychiatric label. This pattern is consistent with 2 additive costs: one associated with the label and the other with the symptoms. Thus, use of a specific psychiatric label, with or without symptoms, increased social distance. In addition, the presence of psychiatric symptoms adds a further increase to desired social distance. In the present study, both the label used and the symptomatology had a significant influence on attitudes, but the interaction between the two was not significant.
The label ‘Si-jue-shi-diao’ (psychosis) is not in use by the medical profession or other organisations in Macao. However, given their close proximity and shared media in Hong Kong and Macao, it is possible that some familiarity with this term is present in Macao. However, it is difficult to be confident with how the new label would have been interpreted by the respondents. When positive symptoms were not present, the social distance expressed towards the label ‘Si-jue-shi-diao’ was the same as the label ‘Jing-shen- fen-lie-zheng’ (the term for schizophrenia). This would suggest that it was interpreted as a serious condition, proving to be as stigmatising as the familiar label ‘schizophrenia’, at least in the absence of symptoms. In contrast, when positive symptoms of schizophrenia were included, the label ‘psychosis’ did elicit lower social distance and perceived risk scores. This suggests that the respondents did view it less negatively than the more familiar psychiatric labels. This supports the idea that a new, unfamiliar label can be less stigmatising.14 It seems reasonable to speculate that the results of the present study would generalise from Macao to Hong Kong. However, this is an empirical question outside the scope of the present study.
In the present study, the gender of the protagonist was manipulated independent of other factors, including the gender of the respondent. In terms of social distance, the gender of the respondent did not have a significant effect on attitudes, whereas significantly greater social distance was expressed towards a male protagonist in the vignette. This is consistent with previous research indicating that female protagonists are generally subjected to less mental illness–related stigma compared with males.15,16 In terms of perceived risk, as well as the significant influence of the gender of the protagonist, the gender of the respondent was also significant. Consistent with previous findings,17 female respondents expressed significantly higher scores than males in terms of perceived risk. These gender-related findings are explicable in terms of the perceived danger and threat of violence associated with mental illness.18,19 Presumably, male protagonists represented a greater risk in terms of potential violence, consequently respondents expressed a desire for greater social distance. Similarly, female respondents presumably felt more vulnerable in relation to a perceived risk of violence and so expressed greater concern compared with male respondents.
In conclusion, the present study supports the idea that psychiatric labels do elicit more negative attitudes compared with a general label ‘illness’. An unfamiliar label (‘Si-jue-shi-diao’) was viewed more positively, but only when positive symptoms were also described. The results suggest that simply focusing on the label alone will not be a successful strategy in terms of combating stigma. Instead, the symptomatology also needs to be addressed, in particular the perceived danger associated with mental illness. This concern is evident from the present results with much higher scores for perceived risk than for social distance (Fig). Although the danger posed by sufferers of mental illness is real, it is far less than the threat perceived by the public.20
The results of the present study suggest that educating people about the risk related to the symptoms of mental illness is an important component to reducing stigma. Although these symptoms can appear disturbing to the general public, they do not inevitably represent danger and are not the antecedents of violence. In fact, the risk posed by sufferers of mental illness is relatively small and, through improved clinical practice, hopefully they are diminishing.21
Acknowledgements
The authors would like to thank to Ms Sin U Leong for her hard work collecting data and the 4 schools in Macao that participated in this study, as well as to Dr Ka-Fai Chung from the University of Hong Kong who generously allowed the authors to use elements of his previous research vignette in the present study.
References
- Lee S, Lee MT, Chiu MY, Kleinman A. Experience of social stigma by people with schizophrenia in Hong Kong. Br J Psychiatry 2005;186:153-7.
- Chung KF, Wong MC. Experience of stigma among Chinese mental health patients in Hong Kong. Psychiatr Bull 2004;28:451-4.
- Corrigan P. How stigma interferes with mental health care. Am Psychol 2004;59:614-25.
- Ono Y, Satsumi Y, Kim Y, Iwadate T, Moriyama K, Nakane Y, et al. Schizophrenia: is it time to replace the term? Psychiatry Clin Neurosci 1999;53:335-41.
- Levin T. Schizophrenia should be renamed to help educate patients and the public. Int J Soc Psychiatry 2006;52:324-31.
- Kim Y, Berrios GE. Impact of the term schizophrenia on the culture of ideograph: the Japanese experience. Shizophr Bull 2001;27:181-5.
- Sato M. Renaming schizophrenia: a Japanese perspective. World Psychiatry 2006;5:53-5.
- Wong GH, Hui CL, Chiu CP, Lam ML, Chung DW, Tso S, et al. Early detection and intervention of psychosis in Hong Kong: experience of a population-based intervention programme. Clin Neuropsychiatry 2008;5:286-9.
- Kingdon D, Vincent S, Vincent S, Kinoshita Y, Turkington D. Destigmatising schizophrenia: does changing terminology reduce negative attitudes? The Psychiatrist 2008;32:419-22.
- Chung KF, Chan JH. Can a less pejorative Chinese translation for schizophrenia reduce stigma? A study of adolescents’ attitudes toward people with schizophrenia. Psychiatry Clin Neurosci 2004;58:507-15.
- 1 Chou KL, Mak KY. Attitudes to mental patients among Hong Kong Chinese: a trend study over two years. Int J Soc Psychiatry 1998;44:215-24.
- Phillips MR, Pearson V, Li F, Xu M, Yang L. Stigma and expressed emotion: a study of people with schizophrenia and their family members in China. Br J Psychiatry 2002;181:488-93.
- Chen C, Lee S, Stevenson HW. Response style and cross-cultural comparisons of rating scales among East Asian and North American students. Psychol Sci 1995;6:170-5.
- Corrigan PW, Watson AC. At issue: Stop the stigma: call mental illness a brain disease. Schizophr Bull 2004;30:477-9.
- Farina A. Are women nicer people than men? Sex and the stigma of mental disorders. Clin Psych Rev 1981;1:223-43.
- Wirth JH, Bodenhausen GV. The role of gender in mental-illness stigma: a national experiment. Psychol Sci 2009;20:169-73.
- Corrigan PW, Watson AC. The stigma of psychiatric disorders and the gender, ethnicity, and education of the perceiver. Community Mental Health J 2007;43:439-58.
- Angermeyer MC, Matschinger H. The stereotype of schizophrenia and its impact on discrimination against people with schizophrenia: results from a representative survey in Germany. Schizophr Bull 2004;30:1049-61.
- Link BG, Phelan JC, Bresnahan M, Stueve A, Pescosolido BA. Public conceptions of mental illness: labels, causes, dangerousness, and social distance. Am J Public Health 1999;89:1328-33.
- Walsh E, Buchanan A, Fahy T. Violence and schizophrenia: examining the evidence. Br J Psychiatry 2002;180:490-5.
- Hinshaw SP, Stier A. Stigma as related to mental disorders. Annu Rev Clin Psychol 2008;4:367-93.
