
East Asian Arch Psychiatry 2014;24:68-74
ORIGINAL ARTICLE
Dr Salleh Mohd Razali, MD, MPM, FAMM, Discipline of Psychological and Behavioural Medicine, Faculty of Medicine, Universiti Teknologi Mara, Sungai Buloh Campus, 47000 Sungai Buloh, Selangor, Malaysia.
Dr Muhammad Zul Azri Mohammad Yusoff, MD, MMed (Psychiatry), Department of Psychiatry General Hospital Kota Bharu, 15200 Kota Bharu, Kelantan, Malaysia.
Address for correspondence: Dr Salleh Mohd Razali, Discipline of Psychological and Behavioural Medicine, Faculty of Medicine, Universiti Teknologi Mara, Sungai Buloh Campus, 47000 Sungai Buloh, Selangor, Malaysia.
Tel: (60-3) 6126 7333; Fax: (60-3) 6126 5224; Email: razali6403@salam.uitm.edu.my
Submitted: 9 October 2013; Accepted: 18 November 2013
Abstract
Objective: Adherence to medication is essential for maximising the outcomes of patients with schizophrenia as the consequences of poor adherence are devastating. The study aimed to compare medication adherence between patients with relapse schizophrenia and those attending psychiatric follow-up clinics, and to determine the factors affecting adherence.
Methods: This was a cross-sectional study involving 70 patients with schizophrenia who were divided equally into 2 groups. Medication adherence was assessed with the Medication Adherence Rating Scale. Appropriate instruments were used to measure insight, social support, and psychopathology. Various socio-demographic and clinical variables were explored to find associations with medication adherence. Results: Medication adherence among patients with schizophrenia was poor; 51% of the patients did not adhere to a medication regimen. Adherence was better in outpatients with schizophrenia (61%) than in relapse cases (39%), although the difference was not statistically significant (t = 1.70; p = 0.09). Besides, relapse patients had significant higher number of admission (X2 = 22.95; p < 0.05) and severe psychopathology (t = –29.96; p < 0.05), while perceived social support was significantly better in outpatients with schizophrenia (t = 2.90; p < 0.05). Frequency of admission (adjusted b = –0.55; 95% confidence interval [CI], -0.99 to -0.10; p < 0.05) and psychopathology (adjusted b = –0.12; 95% CI,
-0.24 to -0.01; p < 0.05) were also significantly associated with medication adherence.
Conclusion: Medication adherence among both groups of patients with schizophrenia was poor. If adherence is addressed appropriately, the number of admissions and severity of psychopathology could be improved.
Key words: Patient compliance; Psychopathology; Schizophrenia; Social support
摘要
目的:药物依从性是使精神分裂症患者达到最佳治疗效果必不可少的因素,因药物依从性欠佳可导致极强破坏性後果。本研究旨在比较精神分裂症复发患者和门诊患者的药物依从性,并检视影响依从性的因素。
方法:这项横断面研究纳入70名精神分裂症患者并平均分为两组,以药物依从性评估量表评估他们药物依从性的程度。研究并使用各种评估工具分别测量他们的洞察力、社会支持和心理病学状况。社会人口学和临床变量则用作探讨与药物依从性的相关性。结果:精神分裂症患者的药物依从性表现欠佳,当中51%患者并无依从药物治疗份量。门诊精神分裂症患者(61%)对药物依从性的表现较复发患者(39%)为佳,但无统计学明显差异(t = 1.70,p = 0.09)。此外,复发患者的入院次数明显较高(X2 = 22.95,p < 0.05),精神病理程度也较严重(t = –29.96,p < 0.05);而门诊精神分裂症患者的感知社会支持也明显较佳(t = 2.90,p < 0.05)。此外,入院次数(经调整b值 =–0.55,95%置信区间 = –0.99至 –0.10,p < 0.05)和精神病理学(经调整b值 =–0.12;95%置信区间 =–0.24至–0.01,p < 0.05)也与药物依从性显著相关。
结论:两组精神分裂症患者的药物依从性皆表现欠佳。如患者能依从药物服用指引,入院次数和精神病理学严重程度均可改善。
关键词:患者依从性、精神病理学、精神分裂症、社会支持
Introduction
Medication adherence or compliance is defined as the extent to which a person’s behaviour coincides with the prescribed medical advice.1 Adherence is best viewed as “continuously disturbed rather than naturally dichotomous”; total adherence or non-adherence is rare.2 Rates of medication non- adherence among patients with schizophrenia vary widely; a figure of up to 90% has been reported, depending on the setting, patient population, and adherence measures.3,4 The majority of experts believe that patients with schizophrenia or bipolar disorder on average takes only 51% to 70% of the prescribed medications.5 Adherence to treatment has a significant impact on the prognosis of schizophrenia. Good medication adherence generally contributes to an improvement in clinical outcome, which leads to a reduced rate of rehospitalisation, higher rates of employment, and improved quality of life and functioning.6
The reasons for poor treatment adherence are complex and heterogeneous.7,8 From patient perspective, these include forgetting to take the medication, losing or running out of medication, thinking that it is not needed, not wanting to take the drug, and fear of side-effects.9 This study aimed to determine the socio-demographic and clinical factors associated with medication adherence in patients with schizophrenia, and compare the difference in medication adherence between currently admitted (relapse schizophrenia) and those attending psychiatric follow- up clinics (outpatients with schizophrenia). Comparison between both groups of patients shall give us an insight into whether medication adherence is the ultimate factor in relapse of the illness.
Methods
Study Subjects and Design
This was a cross-sectional study which used universal sampling to recruit the study sample. Patients with schizophrenia attending psychiatric follow-up clinics and those currently admitted to the psychiatric ward (for relapse of the illness) of Hospital Universiti Sains Malaysia (USM) during the study period were screened for the study. The inclusion criteria were patients meeting the DSM-IV10 diagnostic criteria of schizophrenia and aged between 18 and 65 years. Outpatients with schizophrenia were included provided they had not been admitted in the past 2 years. Patients with co-morbid substance dependence (DSM-IV)10 or mental retardation or who refused to give written informed consent were excluded. Written informed consent was obtained from all patients. The study protocol was approved by the Human Research Ethical Committee of USM. After obtaining socio-demographic and clinical profiles, the selected patients were assessed with the appropriate tools. Outpatients with schizophrenia were assessed at the clinic, while patients with relapse schizophrenia were assessed in the ward as soon as they were stable. Although the same scale was used to assess the medication adherence in both groups, adherences in the relapse cases were referred to the medication adherence behaviour before the present admission, not during the ward stay. This was clarified to the patients in the assessment form. All assessments were performed by the second author (attending psychiatrist).
Rating Instruments
Medication Adherence Rating Scale
Patients’ medication adherence was assessed using a modified Malay version of Medication Adherence Rating Scale (MARS).2 The original MARS is a 10-item self-rating scale with yes / no response. After consulting the original author, only 4 items pertaining to medication adherence behaviour were utilised. They included: (1) “Do you forget to take your medication?” (2) “Are you careless at times about taking your medication?” (3) “When you feel better, do you sometimes stop taking your medication?” and (4) “Sometimes, if you feel worse when you take the medicine, do you stop taking it?”. The other items which are not directly related to medication adherence were not utilised: items 5 to 8 measured the attitudes towards taking medication, and items 9 and 10 assessed negative side-effects and attitude towards psychotropic medications. Total score of MARS ranged from 0 (low likelihood of medication adherence) to 10 (high likelihood).11 For the 4-item scale, a score of ≥ 3 indicated adherence. In the validation study conducted earlier, we found that MARS had acceptable validation indexes. The internal consistency coefficient (Cronbach’s alpha) was 0.75, which was comparable with that of the previous study.2
Insight and Treatment Attitude Questionnaire
The Insight and Treatment Attitude Questionnaire (ITAQ) is an 11-item rating scale to evaluate patient recognition of psychiatric illness and need for treatment, particularly schizophrenia.12 Each question is scored between 0 and 2 with a maximum possible score of 22. Poor insight is associated with a score from 0 to 7, fair insight 8 to 14, and good insight 15 to 22.
Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS) is a 12-item instrument designed to assess perceptions about support from family, friends, and significant others.13 The items are divided into factor groups relating to the source of support, with scores ranging from 1 to 7. High scores indicate high levels of perceived support. In this study, we used a validated Malay version of MSPSS.14 The instrument displayed good internal consistency (Cronbach’s alpha = 0.89) and high test-retest reliability (Spearman’s rho = 0.77; p < 0.001).
Brief Psychiatric Rating Scale
The Brief Psychiatric Rating Scale (BPRS) is an 18-item scale which is divided into psychotic and depressive subscales.15 Each item is scored on a 4-point scale (ranging in severity). There are 6 items in the depressive subscale and another 12 items in the psychotic subscale. The BPRS is widely used to assess the psychopathology of schizophrenia and related psychosis.
Sample Size and Statistical Analysis
The calculated sample size was 30 in each group. All data entries and analyses were processed using the Statistical Package for the Social Sciences (SPSS) Windows version 20. The associations between the demographic data and clinical status of inpatient and outpatient groups were analysed using Pearson’s Chi-square test and independent t test. Association between medication adherence, psychopathology, insight, and perceived social support of inpatient and outpatient groups were analysed using independent t test. Regression analysis was performed to examine the association between insight, perceived social support, and psychopathology with medication adherence.
Results
Socio-demographic and Clinical Characteristics
A total of 70 patients participated in this study, with equal number in each group. The mean (± standard deviation) age of the patients was 33 ± 8 years. Most of the patients were Malays (97%), more than half were male (57%), and the majority was single (63%). Although more than 90% of the patients had either completed secondary school or tertiary education, the majority of them (59%) was unemployed. Therefore, more than half of them (54%) had a monthly income of < 100 Malaysia Ringgit (about 31 USD). Nearly half of the patients (44%) had schizophrenia of >10 years. About half of the patients (53%) had a history of admission of 1 to 5 times. All patients were prescribed antipsychotic medication and about two-thirds (64%) were on atypical antipsychotic drugs.
Group Comparison of Socio-demographic and Clinical Characteristics
The mean age of inpatients and outpatients was 33 ± 10 years and 33 ± 8 years, respectively, and more than half of the participants in both groups were male. There were no statistical differences between the 2 groups in terms of age, gender, education level, marital status, occupation, and personal income. In terms of clinical characteristics, relapse cases had a significantly higher admission rate than outpatients with schizophrenia (X2 = 22.95; p < 0.05; Table 1). However, no significant difference was found in the duration of illness and type of prescribed antipsychotics between the 2 groups.
Group Comparison of Medication Adherence, Psychopathology, Insight, and Social Support
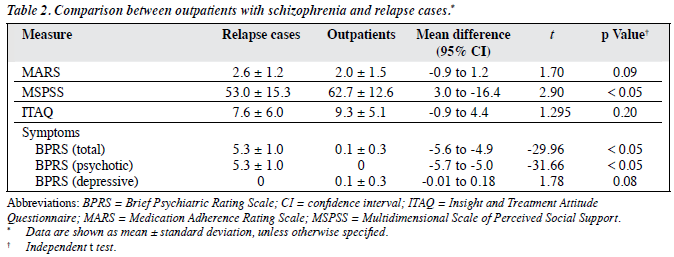
Non-adherence was found in about half of the patients (51%). Specifically, non-adherence in outpatients with schizophrenia was lower (39%) than in relapse cases (61%). However, the difference in medication adherence between the 2 groups did not reach statistical significance (t = 1.70, p = 0.09). In terms of perceived social support, outpatients with schizophrenia had a significantly higher MSPSS score (62.7) than the relapse cases (53.0; t = 2.90, p < 0.05).
Outpatients with schizophrenia had better mean ITAQ scores compared with the relapse cases. In general, the outpatients had fair insight while patients with relapse schizophrenia had poor insight. Although the severity of the psychotic symptoms as measured by the BPRS was relatively low in both groups, the BPRS total score and BPRS psychotic subscore were both significantly higher in patients with relapse schizophrenia than the outpatient group (t = –29.96, p < 0.05; t = –31.66; p < 0.05 respectively). Thus, relapse cases had significantly more severe symptoms than outpatients with schizophrenia (Table 2).
Relationship with Medication Adherence
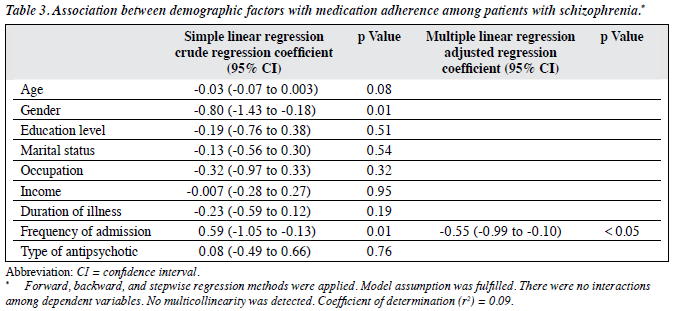
Regression analysis was used to explore the relationship between socio-demographic factors and medication adherence. The relationship was first examined using simple linear regression (SLR). The analysis then proceeded to multiple linear regression (MLR). All the variables that met the initial screening criteria (p < 0.25) were entered into MLR. After controlling for age, gender, and duration of illness, the MLR analysis showed a significant negative linear relationship between the number of admissions and total MARS score. Any admission to a psychiatric ward would reduce the total MARS score by 0.5 (adjusted b = –0.55; 95% confidence interval [CI], -0.99 to -0.10; p < 0.05; Table 3). Therefore, frequency of psychiatric admission accounted for 9% of the MARS total score variance (r2 = 0.09).
The relationships of social support, insight, and psychopathology with medication adherence were explored by regression analysis. The relationships were examined using SLR, followed by MLR. All the variables that met the initial screening criteria (p < 0.25) were entered into MLR. After controlling for insight, the MLR analysis showed a significant negative linear relationship between psychopathology and total MARS score. Increase in the total BPRS by 1 reduced the MARS total score by 0.13 (adjusted b = –0.12; 95% CI, -0.24 to -0.01; p < 0.05; Table 4). Therefore, the severity of schizophrenic symptoms accounted for 8% of the MARS total score variance (r2 = 0.08).

Discussion

This study found a high non-adherence rate in the study subjects, with nearly half of all the patients (51%) not adhering to their medication. As expected, the non-adherence rate among patients with relapse schizophrenia (61%) was higher than that in outpatients with schizophrenia (39%), although the difference in the rate was not significant. Better social support and insight in outpatients with schizophrenia partly contributed to their higher rate of adherence. The non-adherence rate in this study aligns with that from other studies, such as those by Lacro et al16 (49.5%) and Yang et al17 (41.2%). However, one study18 found that the rate of non-compliance with medication was as low as 25.8%.
The poor medication adherence in both groups of patients with schizophrenia in this study is contributed by several local factors, which were not explored in this study. These include subcultural beliefs about mental illness, the interference of Malay traditional healers (Bomoh), and stigmatisation of mental illness. A significant number of psychiatric patients in this country stop taking their medications after visiting traditional healers.19 The stigma towards patients with schizophrenia in developing countries such as Malaysia is also high; it is associated with workplace difficulties, family rejection, follow-up default, and treatment non-adherence.20 A local study21 found that such stigma creates a barrier to modern psychiatric care as the majority of patients prefer traditional treatment.
Recent studies22-24 show that non-adherence to medication was a common factor which predicted the relapse of patents with schizophrenia. On average, non-adherent patients have a 3.7 times greater risk of relapse than patients who adhere to treatment.25 Complete discontinuation of medication is believed to cause about 1 in 10 hospital admissions and 1 in 5 nursing home admissions.26 A local study by Ng et al27 reported that 32.2% of patients who were readmitted to the psychiatric ward of a teaching hospital within 6 months after discharge returned as a result of poor adherence to medication. Poor adherence to medication is the most important factor related to early readmission in patients with psychotic disorders.
Among the socio-demographic variables, only frequency of admission showed a significant difference between the 2 groups; patients with relapse schizophrenia had higher frequency of admission than the outpatients. This finding is in agreement with that from a previous study28 which showed that the number of previous admissions and prescription of multiple antipsychotics were associated with frequent relapse. A local study by Draman et al29 also found that the number of previous admissions was one of the significant risk factors for repeat admissions. It has also been reported that the majority of patients with multiple admissions due to non-adherence to antipsychotic medication early in the treatment is less likely to be adherent later.22 This is in concordance with our finding that the majority of patients with relapse schizophrenia was admitted more than 5 times in the past.
We found that perceived social support was significantly better in outpatients with schizophrenia than patients with relapse schizophrenia. If patients perceived that they were getting adequate social support, the rate of medication adherence was relatively elevated as seen in the outpatient group. Therefore, improving patients’ perceptions of adequate social support might improve medication adherence. This finding was in concordance with the study by Hudson et al30 in which lack of social support and supervision commonly contributed to poor treatment adherence. The medication non-adherence eventually translated to multiple relapses and admissions.
Generally, 50% of patients with schizophrenia have poor insight.31 Their ability to recognise their schizophrenic experiences and label them pathological would improve their insight. This awareness might convince them that they have a mental illness that could benefit from treatment. This, in turn, may lead to improved medication adherence. This hypothesis is supported by other studies32,33 which showed that lack of insight was correlated with poor medication adherence, and a study by Tsang et al34 in which insight was the strongest predictor of medication adherence. However, no statistically significant relationship was found between insight and treatment adherence in this study, although insight was slightly better in outpatients with schizophrenia versus those with relapse. A possible explanation for the non-significant finding might be confounding factors such as duration of illness and chronicity.35 Almost half of the patients in both groups had suffered from schizophrenia for > 10 years. Motivational problems as part of the chronicity of the illness have been cited by Weiden et al36; these will influence clinical attendance rates and adherence to prescribed regimens.
Overall, the relapse patients had significantly more severe psychotic symptoms, with higher mean BPRS score, than the outpatients with schizophrenia. There was also a significant relationship between psychopathology and medication adherence. Patients who had severe psychotic symptoms showed poor medication adherence. It has been shown that the severity of acute psychotic symptoms such as persecutory delusions, hostility, grandiosity, perplexity, and thought disorder is associated with treatment refusal.37,38
It makes sense that those with acute psychotic symptoms of the persecutory variety will be suspicious of treatment or believe that they are being poisoned or punished. Those with grandiosity are unlikely to interpret their mental state as an illness requiring treatment. A recent study by Yang et al17 also found that the severity of disease was closely related with medication adherence. Medication adherence would be poor if patients had more severe psychopathology.
We concluded that if adherence could be addressed appropriately, the number of admissions and severity of psychopathology could be improved, leading to better patient outcomes. In a recent systematic review, Hayness et al39 concluded that current methods of improving adherence for chronic health problems are mostly complex and not very effective, so the full benefits of treatment cannot be realised. In order to improve adherence, the intervention should comprise multiple strategies such as a combination of educational, behavioural, and cognitive strategies.8 The non-adherence rate could also be effectively reduced if simple measures such as prescribing a simple dose regimen (drug dosing not exceeding more than twice per day) and counselling the patients to enhance treatment adherence were implemented routinely in clinical practice.40
This study had several limitations. It was a cross- sectional study with a small sample size; thus, cause- effect relationship could not be determined. A simple method was used to measure medication adherence; a self-rating scale with only 4 items was administered. It is not objective enough to reflect the real picture as we know that medication adherence is a complex issue. There were several other confounding factors which were not assessed such as severity of negative symptoms, side-effects of the medications, complexity of medicine regimens prescribed, and the distance from hospital to home. The sample consisted of a heterogeneous group of patients with regard to chronicity and duration of illness. It is better to limit the duration of the illness to reduce the confounding factors associated with it. Furthermore, more than 90% of the sample comprised Malay patients who did not represent the multiracial society of the country.
Declaration
The authors declared no conflict of interest. The study was self-supported for preparation of dissertation of MMed (Psychiatry), Universiti Sains Malaysia.
References
- Hayness BR, Sackett DL. Compliance with therapeutic regimen. Baltimore: John Hopkins University Press; 1976.
- Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (MARS) for the psychoses. Schizophr Res 2000;42:241-9.
- Corrigan PW, Liberman RP, Engel JD. From non-compliance to collaboration in the treatment of schizophrenia. Hosp Community Psychiatry 1990;41:1203-11.
- Cramer JA, Rosenheck R. Compliance with medication regimens for mental and physical disorders. Psychiatr Serv 1998;49:196-201.
- Velligan DI, Weiden PJ, Sajatovic M, Scott J, Carpenter D, Ross R, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry 2009;70(Suppl 4):1-46.
- Weiden PJ, Olfson M. Cost of relapse in schizophrenia. Schizophr Bull 1995;21:419-29.
- Zygmunt A, Olfson M, Boyer CA, Mechanic D. Interventions to improve medication adherence in schizophrenia. Am J Psychiatry 2002;159:1653-64.
- Razali SM. Prevention of relapse and interventions for enhancing medication adherence in schizophrenia: an East Asian perspective. Asia Pac Psychiatry 2010;2:68-76.
- Cooper C, Bebbington P, King M, Brugha T, Meltzer H, Bhugra D, et al. Why people do not take their psychotropic drugs as prescribed: results of the 2000 National Psychiatric Morbidity Survey. Acta Psychiatr Scand 2007;116:47-53.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed, text revision (DSM IV-TR). Washington DC: APA; 2000.
- 1 Fialko L, Garety PA, Kuipers E, Dunn G, Bebbington PE, Fowler D, et al. A large-scale validation study of the Medication Adherence Rating Scale (MARS). Schizophr Res 2008;100:53-9.
- McEvoy JP, Freter S, Everett G, Geller JL, Appelbaum P, Apperson LJ, et al. Insight and the clinical outcome of schizophrenic patients. J Nerv Ment Dis 1989;177:48-51.
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The Multidimensional Scale of Perceived Social Support (MSPSS). J Pers Assess 1988;52:30- 41.
- Ng CG, Amer Siddiq AN, Aida SA, Zainal NZ, Koh OH. Validation of the Malay version of the Multidimensional Scale of Perceived Social Support (MSPSS-M) among a group of medical students in Faculty of Medicine, University Malaya. Asian J Psychiatry 2010;3:3-6.
- Bech P, Kastrup M, Rafaelsen OJ. Mini-compendium of rating scales for states of anxiety, depression, mania, schizophrenia with corresponding DSM-III syndromes. Acta Psychiatr Scand 1985;326(Suppl):7-37.
- Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry 2002;63:892-909.
- Yang J, Ko YH, Paik JW, Lee MS, Han C, Joe SH, et al. Symptom severity and attitudes toward medication: impacts on adherence in outpatients with schizophrenia. Schizophr Res 2012;134:226-31.
- Nose M, Barbui C, Tansella M. How often do patients with psychosis fail to adhere to treatment programmes? A systematic review. Psychol Med 2003;33:1149-60.
- Razali SM, Khan UA, Hasanah CI. Belief in supernatural causes of mental illness among Malay patients: impact on treatment. Acta Psychiatr Scand 1996;94:229-33.
- Lee S, Chiu MY, Tsang A, Chui H, Kleinman R. Stigmatizing experience and structural discrimination associated with the treatment of schizophrenia in Hong Kong. Soc Sci Med 2006;62:1685-96.
- Razali SM, Najib MA. Help-seeking behaviour among Malay psychiatric patients. Int J Soc Psychiatry 2000;46:281-9.
- Offord S, Lin J, Mirski D, Wong B. Impact of early nonadherence to oral antipsychotics on clinical and economic outcomes among patients with schizophrenia. Adv Ther 2013;30:286-97.
- Caseiro O, Pérez-Iglesias R, Mata I, Martínez-Garcia O, Pelayo-Terán JM, Tabares-Seisdedos R, et al. Predicting relapse after a first episode of non-affective psychosis: a three-year follow-up study. J Psychiatr Res 2012;46:1099-105.
- Schennach R, Obermeier M, Meyer S, Jäger M, Schmauss M, Laux G, et al. Predictors of relapse in the year after hospital discharge among patients with schizophrenia. Psychiatr Serv 2012;63:87-90.
- Fenton WS, Blyler CR, Heinssen RK. Determinants of medication compliance in schizophrenia: empirical and clinical findings. Schizophr Bull 1997;23:637-51.
- Sullivan SD, Kreling DH, Hazlet TK. Noncompliance with medication regimens and subsequent hospitalizations: a literature analysis and cost of hospitalization estimate. J Res Pharm Econ 1990;2:19-33.
- Ng CG, Loh HS, Yee HA, Zainal NZ. The prevalence and associated factors of psychiatric early readmission in a teaching hospital, Malaysia. Malays J Psychiatry 2012;21:1-3.
- San L, Bernardo M, Gómez A, Peña M. Factors associated with relapse in patients with schizophrenia. Int J Psychiatry Clin Pract 2013;17:2-9.
- Draman S, Ismail S, Merchant M, Yusof H, Husin T, Singh SI. A study on risk factors of repeated admissions among patients with schizophrenia in Hospital Kota Bharu, Kelantan, Malaysia. Inter Med J 2005;12:185-92.
- Hudson TJ, Owen RR, Thrush CR, Han X, Pyne JM, Thapa P, et al. A pilot study of barriers to medication adherence in schizophrenia. J Clin Psychiatry 2004;65:211-6.
- Amador XF, Flaum M, Andreasen NC, Strauss DH, Yale SA, Clark SC, et al. Awareness of illness in schizophrenia and schizoaffective and mood disorders. Arch Gen Psychiatry 1994;51:826-36.
- Rocca PB, Marino F, Mongini T, Portaleone F, Bogetto F. Correlation of attitudes toward antipsychotic drugs with insight and objective psychopathology in schizophrenia. Compr Psychiatry 2008;49:170-6.
- Misdrahi D, Petit M, Blanc O, Bayle F, Llorca PM. The influence of therapeutic alliance and insight on medication adherence in schizophrenia. Nord J Psychiatry 2012;66:49-54.
- Tsang HW, Fung KM, Corrigan PW. Psychosocial and socio- demographic correlates of medication compliance among people with schizophrenia. J Behav Ther Exper Psychiatry 2009;40:3-14.
- Nakano H, Terao T, Iwata N, Hasako R, Nakamura J. Symptomatological and cognitive predictors of insight in chronic schizophrenia. Psychiatry Res 2004;127:65-72.
- Weiden P, Olfson M, Essock S. Medication non-compliance in schizophrenia: effects on mental health service policy. In: Blackwell B, editor. Treatment compliance and the therapeutic alliance. Brunswick, NJ: Harwood Academic Press; 1997.
- Marder SR, Mebane A, Chien CP. A comparison of patients who refused and consent to neuroleptic treatment. Am J Psychiatry 1983;140:470- 2.
- Hoge SK, Appelbaum PS, Lawlor T, Beck JC, Litman R, Greer A, et al. A prospective, multi-centre study of patients’ refusal of antipsychotic medication. Arch Gen Psychiatry 1990;47:949-56.
- Hayness RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev 2008;(2):CD000011.
- Razali SM, Yahya H. Compliance with treatment in schizophrenia: a drug intervention program in a developing country. Acta Psychiatr Scand 1995;91:331-5.
