
Hong Kong J Psychiatry 2009;19:82-6
ORIGINAL ARTICLE
華籍老年精神病人在財政決策方面的能力評估的先導研究
FOT Yu, VWC Lui, LCW Lam, HFK Chiu, JHT Karlawish, PS Appelbaum
余靄婷、雷永昌、林翠華、趙鳳琴、JHT Karlawish、PS Appelbaum
Dr Fiona Oi-ting Yu, MBChB, Department of Psychiatry, The Chinese University of Hong Kong, Hong Kong, China.
Dr Victor Wing-cheong Lui,, MRCPsych, LLB, Department of Psychiatry, Tai Po Hospital, Hong Kong
Prof Linda Chiu-wa Lam, MD, FRCPsych, Department of Psychiatry, The Chinese University of Hong Kong, Hong Kong, China.
Prof Helen Fung-kum Chiu, FRCPsych, Department of Psychiatry, The Chinese University of Hong Kong, Hong Kong, China.
Dr Jason HT Karlawish, MD, Division of Geriatric Medicine, University of Pennsylvania, United States.
Dr Paul S Appelbaum, MD, Division of Psychiatry, Law, and Ethics, Department of Psychiatry, College of Physicians and Surgeons of Columbia University, United States.
Address for correspondence: Dr Victor WC Lui, Department of Psychiatry, Tai Po Hospital, 9 Chuen On Road, Tai Po, Hong Kong, China.
Tel: (852) 2607 6111;
Email: victorluiwc@hotmail.com
Submitted: 9 December 2008; Accepted: 21 January 2009
Abstract
Objectives: This was a pilot study exploring the psychometric performance of the Chinese version of the Assessment of Capacity for Everyday Decision-Making questionnaire in financial management among Chinese psychogeriatric patients.
Participants and Methods: The English version of the Assessment of Capacity for Everyday Decision- Making questionnaire was translated into Chinese. Its potential applicability was assessed by 2 focus groups. Eighteen Chinese psychogeriatric patients were recruited. Subjects were administered the Chinese instrument and assessed by independent clinician ratings based on the definition in the United Kingdom Mental Capacity Act 2005.
Results: In the assessment of inter-rater reliability, the intraclass correlation coefficient showed satisfactory reliability for the ability scores of understanding (0.99), appreciation (0.97), reasoning (0.99) and expressing a choice (0.85). The internal consistency, as measured by Cronbach’s alpha, was 0.83 for understanding and 0.86 for reasoning. The ability scores of understanding and reasoning correlated with the clinician ratings.
Conclusion: For this pilot study, the reliability of the Assessment of Capacity for Everyday Decision- Making Ability questionnaire for Chinese older patients was satisfactory. This instrument warrants further evaluation for its validity and applicability in other Chinese populations.
Key words: Cognition disorders; Decision making; Geriatric assessment; Mental competency; Neuropsychological tests
摘要
目的:本先導研究旨在探討在量度華籍老年精神病人在財政決策方面,「日常決策能力評估問卷」中文版的心理測量特性。
參與者與方法:把「日常決策能力評估」英文版問卷翻譯成中文。由兩個專家小組評估其應用能力,並邀請18位老年精神病患者參與評估中文版問卷。臨床精神科醫生則根據2005年英國精神能力法令評估給參與者作獨立評估。
結果:評分者信度方面,組內相關系數於以下幾項能力分數有滿意信度:理解 0.99、鑒識 0.97、理據0.99、表達意願0.85。內部一致性方面,理解和理據的Cronbach’s alpha分別為 0.83和0.86。理解和理據的能力分數與臨床醫生的評估結果相關。
結論:本初步研究發現,「日常決策能力評估問卷」對華籍老年人有滿意的信度,可以把這工具應用至其他華籍人士。
關鍵詞:認知障礙、決策、老年人評估、精神能力、心理測驗
Introduction
The assessment of mental capacity for the management of financial issues is an emerging clinical concern. Clinical judgement regarding mental capacity for money management can have substantial clinical and medico-legal implications, including the use of guardianship orders. Studies suggest that clinical impressions as a basis for concluding that cognitively impaired patients have mental capacity may be limited.1,2 There is a need for proper and thorough documentation of capacity assessment. In this regard, there is a lack of a locally validated structured assessment tool specifically for decision-making capacity in this area.
Existing assessment tools for financial capacity assess problem-solving abilities and are mainly task-oriented. None of them effectively or specifically address capacity to make decision with regard to activities of daily livings.3 The MacArthur Competence Assessment Tools for Treatment (MacCAT-T) and for Clinical Research (MacCAT-CR) were recently recommended as the standard instruments for measuring capacity to consent to treatment and research.4 Based on the framework of the MacCAT-T and MacCAT- CR, a novel instrument to measure everyday decision- making capacity, known as the Assessment of Capacity for Everyday Decision-Making (ACED), was developed to fill this gap.3
The ACED was developed for assessment of everyday decision-making in a western population of older adults with very mild-to-moderate late-life cognitive impairment. It entails a structured interview format to discuss the patient’s problems in performing instrumental activities of daily living and the possible solutions to managing them. Its reliability and validity were recently reported. This study reports the development of the Chinese version of the ACED and its potential applicability in assessing mental capacity to make financial decisions in a group of Chinese psychogeriatric patients in Hong Kong.
Methods
Subjects
Chinese subjects aged more than 60 years were recruited from the inpatient unit of the Department of Psychiatry, Tai Po Hospital, Hong Kong. Subjects with profound communication difficulties were excluded. One of the team’s psychiatrists explained the details of study, assessed the person’s mental capacity to participate in this research, and obtained written informed consent from each participant. The study was approved by the institutional ethical review board.
Among subjects, we recorded whether a knowledgeable informant (a family member or caregiver working in the place where subjects lived) had noted any impairment in financial management. Hence, the subjects were divided into those who had no reported impairments in financial management versus those who had.
Assessment
Measurement of Capacity to Make Financial Decision
The Chinese version of the ACED was the first semi- structured interview developed to assess everyday decision- making capacity in the Chinese population. The English version was reported to have satisfactory reliability and validity.3 The interview template of the ACED has been published previously.3,5 The 4 dimensions of decision- making capacity (understanding, appreciation, reasoning, and expressing a choice) were adapted from the MacCAT-T, of which the Chinese version has been reliably measured and found applicable to a Chinese older population.6 In this study, the ACED interview was translated into Chinese. The Chinese ACED was back-translated to English by an independent bilingual research assistant. The back- translated version was then compared with the original English version by another bilingual psychiatrist.
Like the original, the Chinese ACED has 3 versions for different activities of daily living. These include preparing meals, managing medications, and managing money. Our study was focused on the activity of managing money. Two focus groups were organised to evaluate the comprehensiveness, relevancy, and cultural appropriateness of the Chinese ACED. One group consisted of 2 psychiatrists, 2 occupational therapists, a medical social worker, and a physiotherapist. The other consisted of 5 normal elderly persons in the community. Focus group discussions were held separately to eliminate the possible influence of one group on the other.
Following suggestions, 2 local modifications were made. First, the option “someone could double-check how you spend your money” was changed to “someone whom you trust could plan the spending of your money for you”. Second, the option “someone else could manage your money completely” was changed to “someone whom you trust could manage your money completely”. The above changes were made because the financial issues appeared to be sensitive in the local context and double-checking is not thought to be a common practice in the local elderly population. This adjustment of the phrasing was not considered to result in a significant change in the decision-making abilities being assessed. In contrast to the western studies involving the administration of ACED instrument, written information sheet was not provided to subjects, as a significant proportion of our subjects were illiterate. To standardise the administration of the ACED and minimise the effect of memory impairment, the information given orally was repeated up to 3 times.
As in the original version, the interview schedule of the Chinese ACED entailed: understanding the problem, appreciating the problem, understanding the options to solving the problem, understanding the benefits and harms of the options, appreciating the benefits and harms of the options, expressing an initial choice, comparative reasoning and consequential reasoning about that choice, logical consistency and expressing a final choice.
The Chinese ACED was administered to each subject by a psychiatrist. Relevant non-verbal communication was recorded. The Chinese ACED was a semi-structured interview that provided relevant information on money management for patients and evaluated mental capacity along 4 dimensions, as follows. ‘Understanding’ is the ability to comprehend basic information about a problem, its potential solutions, and the risks and benefits associated with those solutions. ‘Appreciation’ is the ability of a person to recognise how a problem or solution pertains to his or her specific situation. ‘Reasoning’ is the ability to process the information in a logical fashion toward a decision. ‘Expressing a choice’ is the ability to communicate the subject’s decision. Each dimension yields respective ability scores. No single ACED total score is calculated, because significant deficits in even one dimension may result in mental incompetence, even when performance on other dimensions is intact. For subjects with no impairment in money management, the appreciation subscale was omitted because the concept of appreciating one’s problem and the need for a solution does not apply to these subjects. The ACED was administered to 15 subjects and rated by 2 psychiatrists for the assessment of inter-rater reliability.
Clinician Ratings
To evaluate the clinical significance of ACED scores, mental capacity to make financial decisions was independently assessed by the psychiatrist in charge of the patient. The case psychiatrist was blinded to the ACED scores. A dichotomous judgement (i.e. whether the subject was mentally capable or incapable of making financial decisions) was made based on the criteria in section 3 of Mental Capacity Act 2005, United Kingdom. The Act stipulates that persons are unable to make decisions for themselves if: “(a) they are unable to understand the information relevant to the decision; (b) they are unable to retain that information; (c) they are unable to use or weigh the information; or (d) they are unable to communicate a decision.”
This criterion was adopted in our study as it is explicit and consistent with contemporary approaches to the assessment of mental capacity in making financial decisions.
Cognitive Assessment
The Cantonese version of the Mini-Mental State Examination (MMSE) was administered to each subject.5 The MMSE is widely used in clinical practice for psychogeriatric patients and the resulting scores can be used to assess global cognitive ability in Chinese elderly.6
Procedure
All subjects were assessed by a trained psychiatrist. Demographic and clinical data were recorded. The case psychiatrist independently evaluated whether the subjects were impaired with respect to money management by clinical interview and review of hospital records. Informed consent forms were signed by all subjects. The Chinese ACED and Cantonese version of the MMSE were administered to all subjects, following which the case psychiatrist independently rated the subjects as mentally capable or incapable of making financial decisions.
Data Analyses
Data analysis was performed using the Statistical Package for the Social Sciences (Windows version 14.0; SPSS Inc, Chicago [IL], US). An alpha level of 0.05 was considered statistically significant. Intraclass correlation coefficients were calculated to assess the inter-rater reliability of the ACED. The internal consistency of each dimension of the ACED was examined by calculating the Cronbach’s alpha. To understand the clinical significance of the ACED ratings, Spearman’s correlation coefficients between the ACED ability scores and clinician ratings were calculated. The difference in the ability scores between mentally capable and incapable subjects was evaluated using the Mann-Whitney test. Spearman’s correlation coefficients between the ACED ability scores and demographic and clinical variables and MMSE scores were also calculated.
Results
Demographic and Clinical Characteristics
Of the 24 subjects approached, 18 (75%) agreed to participate and completed the assessment. The male-to-female ratio was 5:4. The mean (standard deviation) age was 71 (8) years. Their median duration of education in years was 6. Their mean (standard deviation) MMSE score was 21 (5). Eleven subjects were considered to have impaired money management abilities. Four were diagnosed with dementia, 8 with depression, 3 with schizophrenia and 3 with other mental disorders.
Assessment of Capacity for Everyday Decision- Making Ability Scores
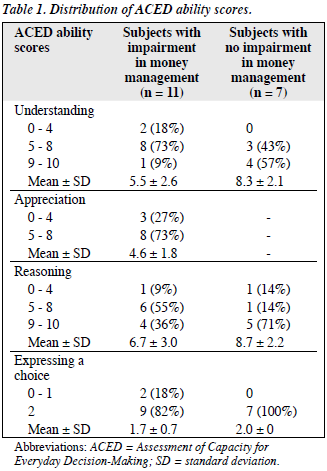
The distribution of the ACED scores for the 4 dimensions is shown in Table 1. Both groups were equally capable of expressing a choice. The ability scores of understanding and reasoning among subjects with no impairment in money management were higher than in those with impairment.
Psychometric Properties of the Chinese Assessment of Capacity for Everyday Decision-Making
Inter-rater Reliability
For all 15 subjects assessed, the intraclass correlation coefficients between the 2 raters were 0.99 for understanding, 0.99 for reasoning, and 0.85 for expressing a choice. For the 11 subjects with impairment in money management, the intraclass correlation coefficient was 0.97 for appreciation.
Internal Consistency
For all 18 subjects assessed, Cronbach’s alpha was 0.83 for understanding and 0.86 for reasoning. For the 11 subjects with impairment in money management, Cronbach’s alpha was 0.59 for appreciation. Internal consistency was not calculated for expressing a choice, because there was only one item in the ACED for this decision-making ability.
Relationship with the Clinician Ratings
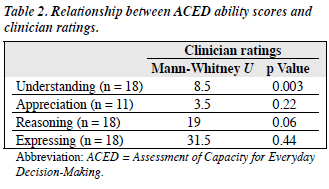
The relationship between ACED scores and clinician ratings is shown in Table 2. The ACED ability scores in understanding and reasoning correlated significantly with the clinician ratings. The understanding scores of mentally capable subjects as measured by clinician ratings were significantly higher than those of mentally incapable subjects (Mann-Whitney U = 8.5, Z = –2.88, p = 0.003). The difference in the reasoning scores approached statistical significance (Mann-Whitney U = 19, Z = –1.96, p = 0.06).
Correlations with Demographic Data and Mini-Mental State Examination Scores
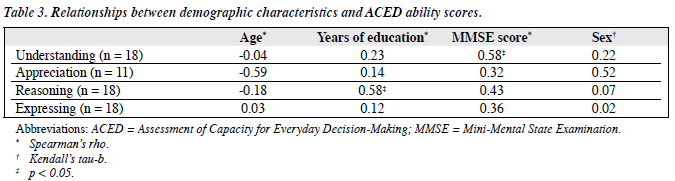
The relationship between ACED ability scores and the demographic data, and MMSE scores is represented in Table 3. Years of education were found to have a significant correlation with the ACED reasoning scores. Moreover, MMSE scores correlated significantly with the ACED understanding scores.
Discussion
Reliability assessment of the Chinese ACED, as assessed by the inter-rater reliability and internal consistency, was satisfactory. This could be due to the highly structured questions and scoring criteria of this instrument. Although larger sample sizes and tests in other populations are needed to confirm these findings, this result supports further evaluation of psychometric properties of the ACED in the local population. The high internal consistency for the 2 ability scores (understanding and reasoning) suggests that a single construct was being measured within each of them. However, among subjects with impairment in money management, internal consistency for appreciation was 0.59. This suggests that the ability to appreciate the problem and possible solutions may be different constructs. In future studies, it would be worth exploring whether the ability to appreciate a problem and appreciate its suggested solution should be analysed separately.
In our study, clinician ratings were used to identify the clinical significance of the ACED ability scores. The correlations between clinician ratings of capacity and ability scores (understanding and reasoning) showed that mentally capable subjects scored significantly higher on the latter measures. In our sample, abilities in understanding and reasoning may exert a greater impact on one’s own decision-making capacity, than the ability to appreciate. Although further study is needed to confirm this finding, these preliminary data support the use of the ACED as a tool for competence assessment. The administration of the Chinese ACED suggests that it can be clinically useful, because most subjects can complete the interview within 15 minutes. It also provides a structured interview format to comprehensively and effectively discuss patients’ money management problems and their solutions.
In keeping with many western studies, there were associations between cognitive impairment and decision- making ability. Understanding scores were positively correlated with MMSE scores. This suggests that the ‘understanding’, as a decision-making ability, might be more affected by cognitive impairment than other decision-making abilities. However, further studies with comprehensive batteries of neuropsychological tests are needed to confirm this speculation.
Interestingly, in our study, years of education correlated significantly with reasoning scores. This relationship with the level of education was not found in another study with the ACED from the West,3 possibly because the education status of our subjects was much lower. A similar relationship between education and the capacity to make treatment decisions was also noted in another local community sample.7 Reasoning ability as measured by the ACED corresponds to the ability to process and manipulate information for decisions. Subjects with low educational attainment may have difficulty in manipulating and processing relevant information for decision-making, which can subsequently affect their performance on a competence assessment. Although this study was not limited to patients with dementia, according to a recent epidemiological study, the educational attainment of Hong Kong patients with mild and very mild dementia was very low.8 The findings of studies from western countries may not be directly applicable to the local Chinese population. It would therefore be worthwhile to further explore the effects of these cultural and education differences on ACED performance and on decision-making abilities in the local population.
Mental capacity has been shown to correlate with clinical features of psychiatric patients. A recent study on psychiatric inpatients found that mental incapacity with respect to making treatment decision was associated with mania, presence of delusional beliefs and poor insight.9 In the present study, the primary objective was to evaluate the psychometric performance of the ACED in Chinese psychogeriatric patients, so correlations with psychopathology were not explored, but may be worth to examining in the future.
This study’s conclusions and further statistical analysis, such as the multivariate analyses, were limited by the small sample size. The lack of any correlation and significant differences may be due to this shortcoming, causing a type II error. The recruitment of the sample was restricted to psychogeriatric inpatients only. Hence, the results should be regarded as preliminary only. Notwithstanding such limitations, the findings support the need for further evaluation of ACED performance in larger samples and in other populations. At the time of writing, this was the first study assessing decision- making capacity for money management in Chinese elderly subjects. A mixed qualitative and quantitative approach was adopted. The findings may provide an impetus for future research in this emerging area of clinical significance.
References
- Marson DC, McInturff B, Hawkins L, Bartolucci A, Harrell LE. Consistency of physician judgments of capacity to consent in mild Alzheimer’s disease. J Am Geriatr Soc 1997;45:453-7.
- Marson DC, Hawkins L, McInturff B, Harrell LE. Cognitive models that predict physician judgments of capacity to consent in mild Alzheimer’s disease. J Am Geriatr Soc 1997;45:458-64.
- Lai JM, Gill TM, Cooney LM, Bradley EH, Hawkins KA, Karlawish JH. Everyday decision-making ability in older persons with cognitive impairment. Am J Geriatr Psychiatry 2008;16:693-6.
- Dunn LB, Nowrangi MA, Palmer BW, Jeste DV, Saks ER. Assessing decisional capacity for clinical research or treatment: a review of instruments. Am J Psychiatry 2006;163:1323-34.
- Lai JM, Karlawish J. Assessing the capacity to make everyday decisions: a guide for clinicians and an agenda for future research. Am J Geriatr Psychiatry 2007;15:101-11.
- Chiu HF, Lee HC, Chung WS, Kwong PK. Reliability and validity of the Cantonese version of the Mini-Mental State Examination: a preliminary study. Hong Kong J Psychiatry 1994;4(Suppl 2):S25-8.
- Lui VW, Lam LC, Luk DN, Wong LH, Tam CW, Chiu HF, et al. Capacity to make treatment decisions in Chinese older persons with very mild dementia and mild Alzheimer’s disease. Am J Geriatr Psychiatry 2009;17:428-36.
- Lam LC, Tam CW, Lui VW, Chan WC, Chan SS, Wong S, et al. Prevalence of very mild and mild dementia in community-dwelling older Chinese people in Hong Kong. Int Psychogeriatr 2008;20:135- 48.
- Cairns R, Maddock C, Buchanan A, David AS, Hayward P, Richardson G, et al. Prevalence and predictors of mental incapacity in psychiatric in-patients. Br J Psychiatry 2005;187:379-85.
