
Hong Kong J Psychiatry 2008;18:6-14
ORIGINAL ARTICLE
Validation of the Chinese Version of the Involvement Evaluation Questionnaire
中文版「評估參與照顧問卷」的心理測量特性
VWK Tang, SK Leung, LCW Lam
鄧穎琦、梁紹裘、林翠華
Dr VWK Tang, MRCPsych (UK), Department of Psychiatry, Castle Peak Hospital, Tuen Mun, Hong Kong, China.
Dr SK Leung, MRCPsych (UK), FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, Castle Peak Hospital, Tuen Mun, Hong Kong, China.
Prof LCW Lam, MRCPsych (UK), FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, The Chinese University of Hong Kong, Territories, Hong Kong, China.
Address for correspondence: Dr Victoria WK Tang, Department of Psychiatry, Castle Peak Hospital, Tuen Mun, Hong Kong, China.
Tel: (852) 2456 7111; Fax: (852) 2463 1644; E-mail: vwktang@gmail.com
Submitted: 22 August 2007; Accepted: 27 September 2007
Abstract
Objective: To validate the Chinese version of the Involvement Evaluation Questionnaire in assessing the caregiving experience for carers of patients with schizophrenia.
Participants and Methods:The Involvement Evaluation Questionnaire was translated into Chinese and back-translated to English. Two hundred and one patients with schizophrenia and their carers were recruited from a psychiatric clinic. The Chinese version of the Involvement Evaluation Questionnaire and the General Health Questionnaire, and the Cantonese version of the Family Burden Interview Schedule were administered to the carers. The patients were assessed by the Structured Clinical Interview, the Positive and Negative Symptoms Scale, and the Global Assessment of Functioning Scale.
Results: Expert panel review and focus group reported content and face validity; concurrent validity was established with correlation with the General Health Questionnaire and the Family Burden Interview Schedule. Construct validity was supported by factor analysis and correlated with the Positive and Negative Symptoms Scale and Global Assessment of Functioning Scale. The Chinese version of the Involvement Evaluation Questionnaire showed substantial correlation with all the rating scales. It showed a significant positive correlation with the Positive and Negative Symptoms Scale and Family Burden Interview Schedule, and a negative correlation with the Global Assessment of Functioning Scale (p < 0.001). The questionnaire demonstrated high test-retest reliability (intraclass correlation coefficient = 0.97; 95% confidence interval = 0.92-0.99), inter-rater reliability (intraclass correlation coefficient = 0.94; 95% confidence interval = 0.86-0.97), and internal consistency (Cronbach's alpha = 0.82).
Conclusion:The psychometric properties of the questionnaire are satisfactory for assessing the care giving experience among carers for the local Chinese population with schizophrenia. Further study is required to demonstrate the questionnaire's sensitivity to change and predictive validity.
Key words: Caregivers; Psychometrics; Questionnaire; Schizophrenia
摘要
目的:檢視中文版「評估參與照顧問卷」用作評估精神分裂病人照顧者的照顧經驗的心理測量特性。
參與者與方法: : 把「評估參與照顧問卷」的原文翻譯成中文,再重新翻譯成英文。一所精神科診所內共201 位精神分裂患者及其照顧者參與研究。把中文版「評估參與照顧問卷」及「一般健康問卷」 以及廣東話版「家庭負擔會談量表」給予照顧者作答。另外,使用「臨床會診量表」、「陽性和陰性症狀量表」、和「功能總體評定量表」評估精神分裂患者。
結果:焦點小組及專家小組報告內容及內容效度。同時效度與「一般健康問卷」和「家庭負擔會談量表」相關。因素分析支持構想效度,並與「陽性和陰性症狀量表」和「功能總體評定量表」相關。中文版「評估參與照顧問卷」與本研究的全部量表存在實質的相關性。它與「陽性和陰性症狀量表」和「家庭負擔會談量表」有顯著正相關,且與「功能總體評定量表」有顯著負相關(p < 0.001 )。這問卷有高重測信度(組內相關系數=0.97; 95%置信區間= 0.92-0.99) 、高評分者信度(組內相關系數= 0.94; 95%置信區間=0.86-0.97)、及高內部一致性(信度系數= 0. 82) 。
結論:中文版「評估參與照顧問卷」用作評估精神分裂病人照顧者的照顧驗酸的心理測量特性令人滿意,須進一步研究這問卷改變的敏感性及預湔測效度。
關鍵詞:照顧者、心理測量特性、問卷、精神分裂
Introduction
Interest in the field of caregiving can be broadly divided into stages. In the 1960s, Grad and Sainsbury2 addressed the effects of the caregiving burden on the community. Hoenig and Hamilton3 were the first to differentiate between objective and subjective burden. Objective burden refers to the observable symptoms, behaviour and disruption to the family, social relations, and household life.4 It includes chores a relative takes on for the patient and also a carer’s supervision and help and cost in terms of career or hobbies foregone in the care process, the ‘dos’ and ‘don’ts’ of caregiving according to Gubman et al.5 Subjective burden refers to the mental health and personal distress aroused in carers in the course of fulfilling their caregiving. This is often in the form of guilt, anger, frustration, grief, depression, hate, and withdrawal.6, Schene et al8 stated that when care between 2 adults is unbalanced, with one party failing to fulfil the reciprocal obligations, care becomes caregiving. In recent years, there was a move away from the negative and stigmatising aspects of caregiving to recognising some more positive aspects of caregiving.9 The emphasis was shifted towards the carer’s needs and mental health, incorporating the physical, emotional, social, and financial needs and coping style into a multidimensional model of caregiving.10
In order to assess the caregiving experience in the local population, a validated assessment tool is needed. Various instruments have been developed to measure the carer burden in relatives of schizophrenia patients, differing in purpose, content, and psychometric properties. Schene et al11 did a study of 21 burden instruments in 1994. However, most of the rating scales used were interviewer-administered, which made them costly and time-consuming. The Involvement Evaluation Questionnaire (IEQ) was chosen because it is a simple and valid, self-administered questionnaire, which is easy to understand and can be administered as a structured telephone interview. It was developed based on a variety of instruments developed in earlier years, covering most domains of the caregiving experience, and focusing on objective measures. It targets a limited time frame and is sensitive to change. The IEQ has been translated into 5 European languages in a large multicentre study, the European Psychiatric Services: Inputs Linked to Outcome Domains and Needs (EPSILON).12 This showed cross- cultural validity and reliability in different centres after translation and also demonstrated a good response rate of 0 to 80%. It can be administered to any type of carers (even friends and neighbours) having more than 1 hour of contact per week with the patient.
Methods
Patients were recruited from the Tuen Mun Mental Health Centre, which serves the population of the New Territories West Cluster of the Hong Kong Hospital Authority. Approval for translation was granted by the original author of the IEQ, Professor AH Schene, and the entire study was approved by the Ethics Committee of the New Territories West Cluster of the Hong Kong Hospital Authority.
Setting
The Tin Shui Wai / Yuen Long area is situated in the north- western part of Hong Kong. According to the 2001 census, it is a growing suburb with a population of 449,0 0 (6. % of the total population), recording 95.5% growth in the past 10 years, due to new migrants settling in the area.13 Of all the districts in Hong Kong, it has the youngest median age and constitutes a low-to-middle class suburb.
Participants
This was a cross-sectional study. A list of all outpatients residing in the Yuen Long / Tin Shui Wai catchment area with a primary diagnosis of F20 to F25 according to the International Classification of Diseases, 10th revision (ICD- 10) classification of mental and behavioural disorders,14 who were active cases of Tuen Mun Mental Health Centre in December 2006, was generated from a centralised computer register. The recruitment period was between February and July 200 . Case notes and computer records were reviewed for eligible patients. The diagnoses were first made by case psychiatrists and a consensus agreed upon in team meetings with supervisors.
Subjects were recruited if they met the following criteria: aged 18 to 65 years; schizophrenia as defined by the ICD-10 classification of mental and behavioural disorders; ethnic Chinese; living at home where at least 1 carer was Chinese and over 18 years old. In addition they had to be able to give informed consent to participate in the study and consent to the interview of a named carer. As the purpose of the study was to examine the psychometric properties and correlates of patients with schizophrenia, subjects were excluded if they were alcohol or drug abusers in the last year, or if they fulfilled an ICD-10 diagnosis for any organic mental disorder, mental retardation, primary dementia, or had any chronic physical illness.
After review of case notes, eligible subjects were contacted over the phone and the purpose of the study was explained. If contact could not be established, patients were approached when they next attended the outpatient department. If consent was obtained, an interview was arranged, mainly on the follow-up date in a consultation room in the outpatient department, at home, or on the ward (for inpatients). Written consent was obtained before the interview from both the patient and the carer. A subgroup of patients and carers was invited for the focus group discussions. The principal researcher administered the rating scales to both the patients and the carers. The Chinese version of the IEQ (C-IEQ) was completed by the carers on their own, whilst the patients were being interviewed. If the carers were illiterate, the questionnaire was read aloud to them item by item by the principal researcher, and the responses recorded. For patients who did not participate in the study, their age, gender, area of residence, education level, and known duration of the illness were obtained from their records.
Assessment Tools
For the Carer Group
The IEQ covers most domains of caregiving consequences. It was developed in the Netherlands from an extensive literature review extending over 40 years and a review of existing instruments. The core module of the IEQ measuring the ‘caregiving consequences’ section comprises 31 items, which focus on the objective aspects of the carer’s experience. The scale is divided into 4 broad groups: tension (strained interpersonal atmosphere between patient and carer), supervision (guarding the patient’s adherence, sleep, and dangerous behaviour), worrying (painful interpersonal cognitions, e.g. concerns and worries about the future), and urging (encouragement and care to motivate and activate the patient to do things for himself / herself). All items are scored on 5-point Likert scales, with higher scores indicating higher carer stress. Internal consistency of the IEQ is high with Cronbach’s alpha of 0.8 to 0.91, and has good test- retest reliability with an intraclass correlation coefficient (ICC) of 0.83 to 0.90.15
Socio-demographic characteristics of the carers were obtained from extension modules of the IEQ. They included: age, gender, educational level, marital status, living arrangements, employment status, relationship to the patient, duration of caregiving, the number of hours spent with the patient per week, financial situation, and general psychological distress based on responses to the General Health Questionnaire (GHQ). The entire set of questions took about 20 to 30 minutes to complete; 10 minutes was needed for the IEQ module alone.
The IEQ was translated into Chinese by a bilingual psychiatrist and back-translated to English by a bilingual master-degree graduate. The back-translated version was compared with the original English version by the author and 3 senior psychiatrists. The modified version was then reviewed by a multidisciplinary expert panel for relevance, accuracy of representation of the items, concepts covered by the questionnaire, and translation accuracy. The panel consisted of 10 healthcare professionals, including therapist, medical social workers, and psychiatrists. Further amendments were made before review by a focus group, which comprised key carers, patients and healthcare professionals, who assessed the translated questionnaire’s cultural appropriateness and acceptability, practicality, and face validity. After final modification, the C-IEQ was pilot- tested on 5 carers, with a focus on clarity and practicality of administration, and no further modification was deemed necessary.
The carers were asked to complete the C-IEQ. Twenty carers were asked to complete the questionnaire again after 10 to 14 days to investigate test-retest reliability. Since the IEQ could be administered as a structured phone interview, the C-IEQ was read to carers who were illiterate. Inter-rater reliability was established by recording 20 such interviews for assessment and rating by an independent researcher, who was a psychiatrist in the same centre. The scores were then compared.
The GHQ is a well-validated self-administered instrument to screen for psychiatric morbidity in the community.16 The 12-item Chinese version was used in this study,1 and was used to demonstrate its concurrent validity for identifying general emotional distress in the carer.
The Family Burden Interview Schedule (FBIS) is a 25-item semi-structured interview developed by Pai and Kapur to assess the burden of care on the family.18 It measures both objective and subjective burden. It has been validated and used in Chinese carers of patients with mental illness.19,20 The Cantonese version of the interview, which has been validated, was used to establish concurrent validity of the C-IEQ. Its internal consistency was good (Cronbach’s alpha being 0.90), and it has good test-retest and inter-rater reliabilities.
For the Patient Group
Socio-demographic features including age, gender, marital status, educational level, employment status, and clinical characteristics (such as age at onset of mental illness, duration of treatment, and number of hospital admissions) were obtained by reviewing case notes.
The Global Assessment of Functioning Scale (GAF) is a 100-point single-item rating scale, indicating overall psychosocial functioning on a continuum from mental health to mental illness from the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV).21 It covers psychological, social, and occupational functioning, and can incorporate information derived from any clinical source, and provides an overall assessment of functional level in the past 1 month. It is a well-validated instrument.22 The GAF scores were correlated with C-IEQ scores.
The Positive and Negative Symptoms Scale (PANSS) measures the severity of psychopathology of patients with schizophrenia, schizoaffective disorder, and other psychotic disorders.23 It comprises 3 scales and 30 items — items for the positive scale, for the negative scale, and 16 for general psychopathology. Its validity and reliability rating Cronbach’s alpha values of 0. 3, 0.83, and 0.8 for the positive, negative, and general psychopathology scales respectively.24 The results were correlated with the C-IEQ scores.
The Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) is a semi-structured interview to obtain reliable corresponding diagnoses.25 The Chinese version has been validated and shows good reliability and agreement (0. 5) between the rater and clinician diagnoses,26 and was used to confirm diagnoses for both the patients and the carers.
Data Analysis
Data analysis for the psychometric properties of the C-IEQ was performed using the Statistical Package for the Social Sciences (Windows version 12.0; SPSS Inc, Chicago [IL], US).
Construct and concurrent validity was examined by calculating the scale-scale correlation of the C-IEQ with the PANSS, GAF, and GHQ scores. The Pearson product- moment correlation coefficient was used for normally distributed continuous variables, and the Spearman rank order correlation coefficient (2-tailed) for those that were not normally distributed. Cronbach’s alpha was estimated for internal consistency of the C-IEQ. Exploratory factor analysis was performed with principal component analysis to delineate the clustering of questionnaire items.
The ICC was used to calculate the test-retest reliability and inter-rater reliability between the different domains and the total score. Individual items were calculated with Cohen’s kappa. The Spearman-Brown prophecy statistic was used to estimate the split-half reliability.
The socio-demographic characteristics of the subjects were summarised using descriptive statistics. The characteristics of those who agreed to be studied were compared to those who refused; the χ2 test was used for categorical data, independent sample t tests for normally distributed variables, and the Mann-Whitney U test for non-normally distributed data. The relationship between the various components of the caregiving domains in the C-IEQ and socio-demographic characteristics was similarly compared. Statistical significance was set as p < 0.05. In situations when corrections for multiple comparisons were required, Bonferroni adjustments were made, in which case a p value of < 0.001 was accepted as statistically significant.
Results
Of the 2,380 patients generated from the list, 1,624 were excluded. Of those excluded, 204 were aged below 18 or above 65 years, 425 had chronic physical problems, and 163 had a history of active substance or alcohol abuse or had co-morbid diagnoses of mental retardation; 250 lived alone, 325 lived in residential homes, 30 had moved to another area or were lost to follow-up, 16 were only living with children who were younger than 18 years; 10 died before recruitment, and 201 were excluded as their diagnoses did not conform to schizophrenia (based on a consensus of diagnosis between the case psychiatrist and another senior psychiatrist). Of the 56 eligible patients, 210 patient-carer dyads agreed to take part in the study. Reasons of refusal included having no interest to participate in the study, carer at work and inability to attend the interview, or not willing to let the carer know about the illness. Nine of the patients were excluded, after SCID was performed and yielded diagnoses other than schizophrenia (Figure).

Patient Characteristics
A total of 201 (2 %) patients participated in the study, 546 (73%) did not. There were no significant differences between the age, gender, area of residence, years of education, and duration of illness of subjects interviewed and those who were not. Of the 201 patients interviewed, 119 (59%) were female and 82 (41%) were male. Their mean age was 40 (standard deviation [SD], 11; range, 18-65) years. The majority of patients (68%) were unemployed. Over half (54%) of them were single; 43% were married. The mean duration of the illness was 15 (SD, 2; range, 1-41) years.
Carer Characteristics
Of the 201 carers interviewed, 114 (5 %) were female and 8 (43%) were male. Their mean age was 53 (SD, 15; range, 19-86) years. Over half (62%) were unemployed; 2% were married. Almost half (45%) of the carers were parents and 3 % were spouses. The mean duration of caregiving was 13 (SD, 9; range, 1-48) years.
Socio-demographic Characteristics
The median monthly domestic household income was HK$ ,000, compared with the area median of HK$16,000. There was an over-representation of residents from public housing units (51%), compared with the territory-wide figure of 31%.
Psychometric Properties of the Chinese version of the Involvement Evaluation Questionnaire
Validity
The expert panel review found the cultural appropriateness of the C-IEQ to be good with 80 to 100% agreement between panel members. Only question (Q.) 14 in the supervision subscale did not achieve a high level of agreement. This question addressed the frequency of disturbed carer sleep, which was loaded on 2 subscales in the original scale structure. It was deemed to have only 60% relevance in the supervision category, but to be highly relevant (100% agreement) in the tension category.
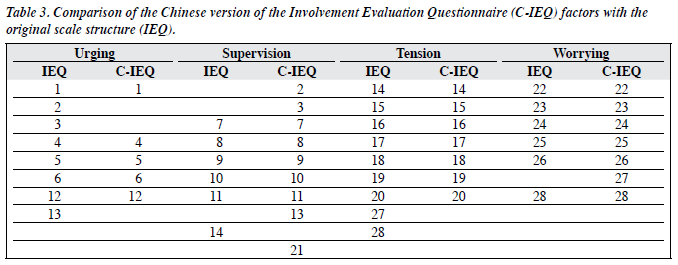
Total C-IEQ scores showed significant positive correlations with the GHQ, PANSS, FBIS, and significant negative correlations with the GAF, based on the Pearson correlation test (Table 1). Exploratory factor analysis was performed after suitability of the data was assessed. The correlation matrix revealed the presence of all item– total coefficients greater than 0.4 (range, 0.42-0.75). The Kaiser-Meyer-Oklin value was 0.83, consistent with good sampling adequacy. The Bartlett’s test of sphericity reached statistical significance, indicating non-identical matrix and factorability. comparability, a 4-factor solution was used for principal component analysis with varimax rotation on factors with eigenvalues greater than 1. This yielded a structure which explained 4 .3% of the variance. Most of the components had reasonably strong loadings (> 0.4), with the exception of Q.13 (0.30) on ‘encouraging the patient to get up’. Each item was loaded on the highest scoring factor. This structure was largely similar to the original scale structure, congregating in 4 factor components (‘supervision’, ‘tension’, ‘urging’, and ‘worrying’). Seven of the questions were loaded in different subscales (Table 2). Q.2 (on helping patients take proper care of themselves), Q.3 (on encouraging patients to eat enough) and Q.13 (on encouraging patients to get up) were grouped under ‘supervision’ instead of ‘urging’. Q.14 (on the frequency of patient disturbing sleep of the carer) was originally weighted on both ‘tension’ and ‘supervision’ scales, was reloaded but only on the ‘tension’ scale. Q.21 (about the time the carer had to pursue his / her own activities), which was not on the original scale, was loaded under ‘supervision’. Q.2 (on worries about the carer’s own future) and Q.28 (on the extent of patient’s mental health problem being a burden) both weighed on ‘worrying’ instead of ‘tension’ (Table 3). Scores of each of these factors in the C-IEQ also showed significant positive correlations with PANSS, GHQ and FBIS, and negative correlations with the GAF (Table 4).



Reliability
The Cronbach’s alpha estimating internal consistency of the C-IEQ was 0.82. The split-half reliability was examined by dividing the questionnaire items into 2 halves by random numbers. The Spearman-Brown coefficient was 0.86. The test-retest reliability was calculated as kappas, which ranged from 0.69 to 0.84 for individual test items and an ICC of 0.97 with 95% confidence interval of 0.92 to 0.99 for the total score. Inter-rater reliability was calculated and yielded kappas of 0. 8 to 1 for individual items, and for the total score the ICC was 0.94 with a 95% confidence interval of 0.86 to 0.9 .
Discussion
These results suggest that the psychometric properties of the C-IEQ were satisfactory in a local Chinese population of patients with schizophrenia. Face validity and content validity were established by an expert panel review and questions, although amendments were made to enhance clarity. The open question at the end of the questionnaire did not show any significant missing domains in terms of carer experience. The pilot test demonstrated applicability and practicality of administration.
Construct validity was examined by hypothesis testing, linking the correlation between stress in the carer to the theoretical constructs of the severity of psychopathology and level of functioning of the patient. Convergent validity was demonstrated by C-IEQ scores showing positive correlations with the PANSS scores and negative correlations with the GAF scores. A Cronbach’s alpha of 0.82 indicated good internal consistency. The inter-rater reliability and test-retest reliability were good with ICC values of 0.94 and 0.9 .
Exploratory factor analysis was performed to examine the hypothesised constructs from the sample. The IEQ was validated in a large multicentre study in 5 European countries aiming to produce a standardised instrument for cross-cultural use. To facilitate international comparison and better applicability, it was decided to preserve a 4-factor scale structure approximating the original. Factor analysis yielded a slightly different factor loading, which incorporated items Q.2, Q.3, and Q.13 into ‘supervision’ instead of ‘urging’. Regarding the Chinese mentality, these are concepts which are more closely linked with basic needs and the practicality of ‘supervision’ than ‘urging’, which is in keeping with the cultural norm whereby Chinese carers had always taken on a supervisory role,2 and are more concerned and anxious about providing actual physical care.28 Some questions, which were originally loaded on 2 subscales, were loaded on 1 only. Thus, Q.14, which was originally weighted on both ‘tension’ and ‘supervision’ scales, was now loaded on ‘tension’ only. Q.28 on both ‘tension’ and ‘worrying’ was now loaded only on ‘worrying’. Q.2 was now weighed on ‘worrying’ instead of ‘tension’. Q.21, which was about the time the carer had to pursue his / her own activities, was not loaded on the original scale but was now loaded negatively on the ‘supervision’ scale, which could be explained by more time being spent on supervisory chores, and less leisure time available for the carer.
In the absence of a ‘gold standard’ for measuring caregiving burden, the GHQ, which measures distress, and the FBIS, which measures the extent of both objective and subjective family burden in various areas, were selected to evaluate concurrent validity. The strong correlation with both the GHQ and the FBIS, the theoretical constructs of general psychological distress and family burden, demonstrate concurrent validity. In particular, the strongest correlation was with the disruption of routine family activities and family interaction noted on the ‘tension’ subscale scores in the C-IEQ, while the disruption of family leisure activities corresponded to the ‘urging’ subscale scores.
Comparison of the pattern of scores with the European studies suggests that the 5-country subscale scores show a similar pattern across different countries; ‘worrying’ was the most frequently mentioned, followed by ‘urging’, ‘interpersonal tension’, whilst ‘supervision’ was mentioned least.29 In the current study sample, using the scale with increased numbers of items under ‘supervision’, the pattern was different, although ‘worrying’ and ‘urging’ were still the most frequently mentioned; ‘supervision’ now superceded ‘interpersonal tension’, which could be attributed to cultural differences. As Chinese society places much emphasis on harmony and integration to maintain stability, it sets great store by patience and forbearance in the face of stress.30 Carers tend to tolerate a patient’s behaviour to avoid conflict or take up chores rather than risk confrontation. This attitude is often reinforced by a sense of moral obligation and resignation to care for any ill relative,31 and therefore renders ‘interpersonal tension’ less prominent and ‘supervision’ more significant.
In this study, several limitations are acknowledged. Sensitivity to change and predictive validity of the C-IEQ were not investigated due to the cross-sectional design. Longitudinal studies are needed to evaluate the predictive validity of the C-IEQ. Confirmatory factor analysis could validate the scale structure for assessing the carer experience. Only patients living with their carers were recruited, although carers not living with their mentally ill relatives could also suffer from significant stress, particularly in terms of worry.32 Patients living alone may be a particularly stable population. Moreover, the high refusal rate due to the double consent required in carer studies may make ours a less representative sample. Even though patients not interviewed had comparable demographics, they could be more stable and require little supervision, hence relatives were able to work and were therefore unavailable to take part in the study. Alternatively, such patients could have refused because they were more paranoid and hostile. In addition, the relatively high percentage residing in public housing and having low household incomes may have limited the generalisability of the results.
As burden is a culture-specific concept, further study engaging subjects from different centres and backgrounds or in other Chinese-speaking regions could help to establish culture-specific threshold scores for detecting carers at risk of significant stress. Moreover, cross-cultural studies could be enhanced by using comparable instruments validated in specific cultural contexts. This questionnaire could be useful in identifying and monitoring the level of stress in carers, and hence facilitate timely intervention and support.
Acknowledgements
The authors would like to thank Prof AH Schene for his kind consent of translation of the IEQ, Prof H Chiu and Dr BWM Siu for permission to use the Chinese version of the SCID and the Cantonese version of the FBIS. We would also like to thank the expert panel and focus group for their help in the study. Thanks also go to all patients and carers who kindly consented to participate in this study. This research is a part of a dissertation for the Hong Kong College of Psychiatrists Fellowship Examination.
References
- Hatfield AB, Lefley HP. Families of the mentally ill: coping and adaptation. New York: Guildford Press; 198 .
- Grad J, Sainsbury P. Mental illness and the family. Lancet 1963;1:544- .
- Hoenig J, Hamilton MW. The schizophrenic patient in the community and his effect on the household. Int J Soc Psychiatry 1966;12:165- 6.
- Platt S. Measuring the burden of psychiatric illness on the family: an evaluation of some rating scales. Psychol Med 1985;15:383-93.
- Gubman GD, Tessler TC, Willis G. Living with the mentally ill: factors affecting household complaints. Schizophr Bull 198 ;13: 2 -36.
- Yarrow M, Clausen J, Robbins P. The social meaning of mental illness. J Soc Issues 1955;11:33-48.
- . Fadden G, Bebbington P, Kuipers L. The burden of care: the impact of functional psychiatric illness on the patient’s family. Br J Psychiatry 198 ;150:285-92.
- Schene AH, van Wijngaarden B, Koeter MW. Family caregiving in schizophrenia: domains and distress. Schizophr Bull 1998;24:609-18.
- Bulger MW, Wandersman A, Goldman CR. Burdens and gratifications of caregiving: appraisal of parental care of adults with schizophrenia. Am J of Orthopsychiatry 1993;63:255-65.
- Chou KR. Caregiving burden: a concept analysis. J Pediatr Nurs 2000;15:398-40 .
- 1 Schene AH, Tessler RC, Gamache GM. Instruments measuring family or caregiver burden in severe mental illness. Soc Psychiatry Psychiatr Epidemiol 1994;29:228-40.
- Schene AH, van Wijngaarden B. Caregiving in schizophrenia: development, internal consistency and reliability of the involvement evaluation questionnaire – European version EPSILON study 4. Br J Psychiatry 2000;1 :S21- .
- 2001 Population census. HKSAR: Census and Statistics Department; 2001.
- The ICD 10 classification of mental and behavioural disorders: diagnostic criteria for research. Geneva: World Health Organization; 1993.
- Schene AH, van Wijngaarden B, Koeter M. Development and reliability of the IEQ-EU. In: Thornicroft G, Becker T, Knapp M, Knudsen HC, Schene A, Tansella M, et al. International outcome measures in mental health. Quality of life, needs, service satisfaction, costs and impact on carers. London: Gaskell; 2006: 92- .
- Goldberg D, Williams PA. User’s guide to the General Health Questionnaire. Windsor: NFER/Nelson; 1988.
- Chan DW. The Chinese version of the General Health Questionnaire: does language make a difference? Psychol Med 1985;15:14 -55.
- Pai S, Kapur RL. Impact of treatment intervention on the relationship between dimensions of clinical psychopathology, social dysfunction and burden on the family of psychiatric patients. Psychol Med 1982;12:651-8.
- Chien WT, Norman I. The validation and reliability of a Chinese version of the family burden interview schedule. Nurs Res 2004;53:314-22.
- Siu BW, Yeung TM. Validation of the Cantonese version of Family Burden Interview Schedule on caregivers of patients with obsessive compulsive disorder. Hong Kong J Psychiatry 2005;15:109-1 .
- Diagnostic and statistical manual of mental disorders, 4th edition. Washington, DC: American Psychiatric Association; 1994.
- Handbook of psychiatric measures, 1st edition. Washington, DC: American Psychiatric Association; 2000.
- Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 198 ;13:261- 6.
- Kay SR, Opler LA, Lindenmayer JP. Reliability and validity of the positive and negative syndrome scale for schizophrenics. Psychiatry Res 1988;23:99-110.
- Williams JB, Gibbon M, First MB, Spitzer RL, Davies M, Borus J, et al. The Structured Clinical Interview for DSM-III-R (SCID). II. Multisite test-retest reliability. Arch Gen Psychiatry 1992;49:630-6.
- So E, Kam I, Leung CM, Chung D, Liu Z, Fong S. The Chinese- bilingual SCID-I/P Project: stage 1 – reliability for mood disorders and schizophrenia. Hong Kong J Psychiatry 2003;13:7-18.
- Ye J, Zhang M, Yao C. Investigations on the burden of family with a schizophrenia patient in five major cities of China. Journal of Clinical Psychological Medicine 1994;4:91-3.
- McCubbin M, McCubbin H. Families coping with illness: the resilience model of family stress, adjustment and adaptation. In: Danielson C, Hamel-Bissell B, Winstead-Fry P, editors. Families, health and illness: perspectives on coping and intervention. St Louis: Mosby; 1993: 21- 63.
- van Wijngaarden B, Schene A, Koeter M, Becker T, Knapp M, Knudsen HC, et al. People with schizophrenia in five countries: conceptual similarities and intercultural differences in family caregiving. Schizophr Bull 2003;29:5 3-86.
- Lee RPL. Cultural tradition and stress management in modern society: learning from the Hong Kong experience. In: Lin TY, Tseng WS, Yeh EK, editors. Chinese societies and mental health. Oxford: Oxford University Press; 1995: 40-52.
- Fung C, Ma A. Family management in schizophrenia. Hong Kong Journal of Mental Health 199 ;26:53-63.
- Laidlaw TM, Coverdale JH, Falloon IR, Kydd RR. Caregivers’ stresses when living together or apart from patients with chronic schizophrenia. Community Ment Health J 2002;38:303-10.
