
Hong Kong J Psychiatry 2009;19:117-20
ORIGINAL ARTICLE
酗酒者與家人在印度家庭中的互動型態
Mr Narendra Kumar Singh, MSW, MPhil (Psychiatric Social Work), Department of Psychiatric Social Work, Central Institute of Psychiatry, Government of India, Kanke, Ranchi-834006, State-Jharkhand, India.
Mr Dipanjan Bhattacharjee, MSW, MPhil (Psychiatric Social Work), Department of Psychiatric Social Work, Central Institute of Psychiatry, Government of India, Kanke, Ranchi-834006, State-Jharkhand, India.
Dr Basudeb Das, MBBS, MD (Psychiatry), Department of Psychiatry, Central Institute of Psychiatry, Government of India, Kanke, Ranchi-834006, State- Jharkhand, India.
Mr Mukul Kumar, MA (Psychology), Department of Clinical Psychology, Central Institute of Psychiatry, Government of India, Kanke, Ranchi-834006, State-Jharkhand, India.
Address for correspondence: Mr Narendra Kumar Singh, Psychiatric Social Work, Junior Psychiatric Social Worker, At-Satya Nand Teaching Block, Central Institute of Psychiatry, Government of India, Kanke, Ranchi-834006, State- Jharkhand, India.
Tel: (91) 9835191942;
E-mail: narendrapsw@gmail.com
Submitted: 5 January 2009; Accepted: 5 March 2009
Abstract
Objective: To assess the interaction patterns in families where the husband has alcohol dependence syndrome.
Participants and Methods: The sample consisted of 30 spouses of men diagnosed with alcohol dependence syndrome and 30 spouses of men with no psychiatric diagnosis and / or alcohol dependence syndrome or any other substance addiction. Purposive sampling was used to select the samples. The Family Interaction Pattern Scale and General Health Questionnaire–12 were used for data collection.
Results: A poorer pattern of family interaction was found in the domains of ‘reinforcement’, ‘social support’, ‘role’, ‘communication’, ‘leadership’, and Family Interaction Pattern Scale total score in spouses of patients with alcohol dependence compared to spouses of people with no alcohol dependence.
Conclusion: There were significant differences in the family interaction patterns displayed by families where the spouse had alcohol dependence and those where the spouse did not have alcohol dependence.
Key words: Alcohol drinking; Family relations; Spouse abuse
摘要
目的:研究丈夫為酗酒者的家庭中的互動型態。
參與者與方法:參與者分為兩組:(1)丈夫為酗酒者的30位配偶,和(2)丈夫並不是酗酒者,沒有精神病,以及沒有其他物質成癮的另外30位配偶。本研究採用立意抽樣方式進行,並 使用「家庭互動模式量表」及「一般健康問卷12」收集數據。
結果:比較兩組的互動型態後,發現配偶為酗酒者的家庭在以下互動型態幾方面較差:鞏固、社會支持、角色、溝通、領導,以及家庭互動模式量表總分數。
結論:配偶為酗酒者和配偶並不是酗酒者的家庭中,其互動型態有顯著分別。
關鍵詞:飲酒、家庭關係、配偶虐待
Introduction
Alcohol dependence, a common psychiatric disorder in the general population, has a significant impact on public health.
In recent years, alcohol dependence has become a major social and personal menace in most societies. According to the World Health Organization (WHO),1 alcohol use disorders accounted for 1.4% of the global disease burden. Globally, alcohol consumption causes 3.2% of deaths (1.8 million) and 4.0% of the disability-adjusted life years lost (58.3 million).2 The WHO also stated that there are causal relationships between alcohol consumption and more than 60 types of disease and injury.2 Along with the costs incurred by alcohol- related illnesses, alcohol dependence contributes substantially to social, financial, and legal problems. Both pathological and chronic alcohol dependence are directly linked to markedly impaired family interactions, and other serious problems like domestic violence and spousal abuse.3-5 Chronic alcohol dependence is associated with interpersonal violence and worsening patterns of interaction. Certain behaviours, such as aggression and impulsivity, are common in people with chronic alcoholic dependence.4-6 Thus, understanding the characteristics of the drinker and the relationship between alcohol dependence and its negative consequences may help to clarify the development and prevention of alcohol-related problems.
Some people are more likely than others to experience the consequences of alcohol use. These tend to be associated with being male7-9; having high perceived stress and anxiety; dissatisfaction with, and poor quality of, life; lack of social support; economic strains; and chronic stress.10,11 In a study done by Frankenstein et al,12 spouses of alcohol-dependent individuals were found to have better problem-solving abilities when the husbands were drinking than when they were not drinking alcohol. Alcohol increased the positive interactions between spouses and alcoholic individuals. In another study, which compared 8 alcoholic and 8 non- alcoholic couples, the alcoholic couples had more negative interaction (hostility, blame, criticism) during the drinking period than the non-drinking period.13
Alcohol has been consumed in India since antiquity. Many mythological texts portray alcoholic beverage drinking by the people of ancient India. The Indian alcohol-drinking pattern has changed dramatically over time. Previously, alcohol use was occasional and had ritualistic connotations; people usually used it during major social events only. But today, the common purpose of consuming alcohol is to get drunk.14 In India, over 20% of all disability-adjusted life years are lost chiefly because of factors like ‘poor health status of the people’ and ‘marked nutritional deficiencies’, as well as ‘high prevalence of alcohol addiction among the people’.15
In northern India, the 1-year prevalence of alcohol use has been estimated as 25 to 40% in the general population, whereas in southern India this rate has been estimated as 30 to 50%. In southern India, the prevalence of alcohol use is higher among people of lower socio-economic status and those who have lower levels of education.15,16 A large-scale survey over 32,000 people performed in 2001 found alcohol use rates of 20 to 38% in males and 10% among females.14
There is a paucity of literature investigating the relationship between family interactions and alcohol dependence. The present study was carried out to examine the family interaction patterns in Indian families with alcohol-dependent persons.
Methods
Design
This was a cross-sectional study examining differences between the interactions of the wives of clinically diagnosed alcohol-dependent men and wives of men with no known psychiatric morbidity and substance dependence, including alcohol dependence. The study was carried out among spouses of patients who came to the ‘De addiction Centre’ of the Central Institute of Psychiatry, a government- owned psychiatric hospital situated in the Ranchi district of Jharkhand State in India. Data were collected for 6 months from March 2008 to September 2008 at the Central Institute of Psychiatry. The study subjects were recruited using the ‘purposive sampling method’.
Inclusion and exclusion criteria were as follows. The experimental group was made up of wives of men diagnosed as having ‘Mental and behavioural disorders due to use of alcohol’ (F10) by consultant psychiatrists from the Central Institute of Psychiatry, defined according to the ICD-10 Classification of Mental and Behavioural Disorders – Diagnostic Criteria for Research (ICD-10 DCR). Only those who had been married for 2 or more years, scored less than 3 in the General Health Questionnaire–12 (GHQ-12), were free from major physical illnesses, and who gave their informed consent to participation in the study were included. The control group were selected after matching their ages, educational and income levels with the experimental group. They also all scored less than 3 in the GHQ-12, did not have major physical illnesses, and gave their informed consent to participation in the study.
Participants
The sample consisted of 30 spouses (wives) of male patients diagnosed with alcohol dependence syndrome (ADS) using the criteria laid out in the ICD-10 (WHO, 199217) by consultant psychiatrists from the Central Institute of Psychiatry, Ranchi, who had no other co-morbidities (either psychiatric, or major physical co-morbidity, or both); and 30 wives of appropriately matched males (control group) with no history of alcohol dependence, who scored less than 3 on the GHQ-12.18
Procedure
Participants completed a socio-demographic data sheet, then were administered the Family Interaction Pattern Scale (FIPS).19 Both groups were given the GHQ-1218 and those who scored below the cut-off (≤3) in the GHQ-1215 underwent further assessments.
Tools
Study tools included a specially designed socio-demographic datasheet, the FIPS19 and the GHQ-12.18 The FIPS, developed by Bhatti et al,19 was used to assess patterns of interaction within couples. This is a scale with 106 items in 6 domains, e.g. ‘reinforcement’, ‘social support’, ‘role’, ‘communication’, ‘cohesiveness’, and ‘leadership’. It measures the family functioning within those 6 domains on a 1-4–point Likert type scale. A higher score shows dysfunction in that sub-domain. It has been shown that this scale is able to effectively measure dysfunction in the families of alcoholics, hysterics and depressives, and has demonstrated satisfactory inter-rater reliability and test- retest reliability.19 The GHQ-12 is widely used to screen for psychiatric distress18 in communities.
Statistical Analyses
Descriptive statistics (percentage, mean, and standard deviation) were used to describe sample characteristics. The Chi-square test was used for describing and comparing categorical data. The independent sample ‘t’ and Mann- Whitney U tests were used to compare continuous variables between these 2 groups.
Results
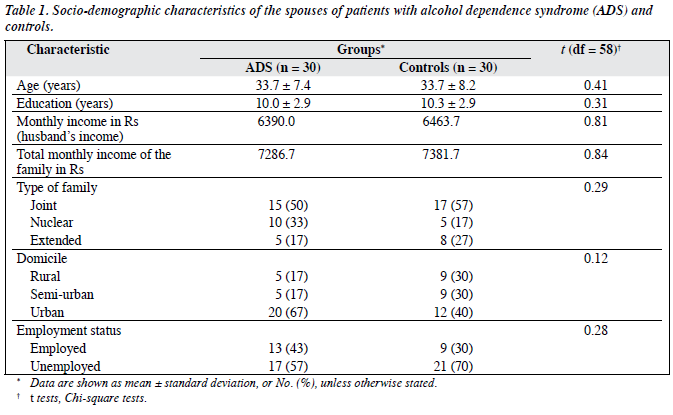
There were no significant differences between the 2 groups in the socio-demographic variables (age, education, family income, spouse’s income, type of family, domicile, and occupation) [Table 1].
There were significant differences between the 2 groups in the FIPS total score and its domains like ‘reinforcement’, ‘social support’, ‘role’, ‘communication’ and ‘leadership’ (Table 2). The mean scores in the above domains were significantly higher in the ADS group (t = 7.8, p < 0.001). No difference could be observed in the ‘cohesiveness’ domain of the FIPS (t = 0.7, p = 0.7).

Discussion
This study was carried out on 60 subjects (30 wives of patients diagnosed with ADS and 30 spouses of men who did not have ADS). The groups were matched for socio- demographic factors. The purpose of the study was to assess the interaction patterns of couples where the husband has ADS. We found that these patterns were dysfunctional. The dysfunction appeared to be pervasive, involving the domains of ‘lack of reinforcement’, ‘poor spousal support’, ‘inadequate role functioning’, ‘unclear and faulty communication pattern’, ‘poor leadership styles’. Impaired interaction patterns manifesting as ‘poor family support and communication’ marred by negative connotations have been highlighted by previous researchers.20-22 Jacob et al13 suggested that alcoholic families differ from non-alcoholic families in ‘affective expression and showing warmth’ to family members. These authors showed that this is reflected as ‘prevalence of lower rates of positive affect and higher rates of negative affect’ in those families. We also found that spouses of alcohol-dependent individuals have marked dissatisfaction with spousal support. In an earlier study, researchers observed that alcoholic couples had more negative communication and attitudes (e.g. criticism, blaming) when drinking than when not drinking.22,23 Poor interactions can have serious implications for drinking behaviour. A person may become more vulnerable to alcohol dependence if exposed to persistent negative communication. On the other hand, his alcohol dependence–related behaviour can force family members to make negative comments.24 Finney et al20 found that positive family interaction patterns, such as a greater sense of emotional closeness or family cohesion and a lack of intra-family conflict, promote healthier levels of alcohol consumption among adults with no chronic dependence.
Our study has some limitations. The sample size is small and is cross-sectional. Important clinical variables like treatment adherence and duration of the illness have not been included. The small sample size means our conclusions are not generalisable. Cultural factors are also important in this issue but the effects of race and ethnicity have not been taken into consideration in this study.
The results revealed significant differences in the quality of the interactions between families with an alcoholic member and those with no alcoholic members. Wives of alcoholic men reported marked problems in almost all areas of family interaction. The present study indicates that marital or family therapy may be an important therapeutic element in the management of ADS.
References
- The World Health Report: World Health Organization. Geneva: Switzerland;
- Global status report: Alcohol policy: World Health Department of Mental Health and Substance Abuse. Geneva: WHO; 2004.
- Caetano R, Cunradi C. Alcohol dependence: A public health Addiction 2002;97:633-45.
- Bell NS, Harford T, McCarroll JE, Senier Drinking and spouse abuse among U.S. Army soldiers. Alcohol Clin Exp Res 2004;28:1890-7.
- Hoffman MJ, Demo DH, Edwards JN. Physical wife abuse in a nonwestern society: an integrated theoretical J Marriage Fam 1994;56:131-46.
- Ohannessian CM, Hesselbrock VM. The influence of perceived social support on the relationship between family history of alcoholism and drinking behaviors. Addiction 1993;88:1651-8.
- Hamilton CJ, Collins JJ The role of alcohol in wife beating and abuse: a review of the literature. In: Collins JJ Jr, editor. Drinking and crime: perspectives on the relationships between alcohol consumption and criminal behavior. New York: Guilford Press; 1981:253-87.
- Jacob T, Seilhamer RA. Alcoholism and family interaction. Recent Dev Alcohol 1989;7:129-45.
- Liban C, Smart Generational and other differences between males and females in problem drinking and its treatment. Drug Alcohol Depend 1980;5:207-21.
- Perkins Gender patterns in consequences of collegiate alcohol abuse: a 10-year study of trends in an undergraduate population. J Stud Alcohol 1992;53:458-62.
- Suman LN, Nagalakshmi Family interaction patterns in alcoholic families. NIMHANS Journal 1995;13:47-52.
- Frankenstein W, Hay WM, Nathan PE. Effects of intoxication on alcoholics’ marital communication and problem solving. J Stud Alcohol 1985;46:1-6.
- Jacob T, Ritchey D, Cvitkovic JF, Blane Communication styles of alcoholic and nonalcoholic families when drinking and not drinking. J Stud Alcohol 1981;42:466-82.
- Mohan D, Chopra A, Ray R, Sethi H. Alcohol consumption in India: a cross-sectional In: Room R, Demers A, Bourgault C, editors. Surveys of drinking patterns and problems in seven developing countries. Geneva: World Health Organization; 2001:103-14.
- Chakravarthy Community workers estimate of drinking and alcohol- related problems in rural areas. Indian J Psychol Med 1990;13:49-56.
- Peters DH, Preker AS, Yazbek AS, Sharma RR. Better health systems for India’s poor: findings analysis and options. Washington DC: The World Bank;
- The international classification of mental and behavioral disorders. 10th revision. Geneva: World Health Organization; 1992.
- Goldberg DP, William A user guide to General Health Questionnaire. Windsor: NFER-Nelson; 1978.
- Bhatti RS, Cuba KDK, Benedicta Validation of Family Interaction Pattern Scale. Indian J Psychiatry 1986;28:211-6.
- Finney JW, Moos RH, Mewborn CR. Posttreatment experiences and treatment outcome of alcoholic patients six months and two years after J Consult Clin Psychol 1980;48:17-29.
- Hagihara A, Tarumi K, Nobutomo Positive and negative effects of social support on the relationship between work stress and alcohol consumption. J Stud Alcohol 2003;64:874-83.
- Sadava SW, Pak Stress-related problem drinking and alcohol problems: a longitudinal study and extension of Marlatt’s model. Can J Behav Sci 1993;25:446-64.
- Hilton ME. Drinking patterns and drinking problems in 1984: results from a general population Alcohol Clin Exp Res 1987;11:167- 75.
- Cunradi CB, Caetano R, Clark CL, Schafer Alcohol-related problems and intimate partner violence among white, black, and Hispanic couples in the U.S. Alcohol Clin Exp Res 1999;23:1492-501.
