
Hong Kong J Psychiatry 2008;18:92-100
ORIGINAL ARTICLE
自動思維問卷(馬來版) 的探索性及驗證性因素的特性和心理計量特性
Dr TPS Oei, PhD, School of Psychology, University of Queensland, Brisbane, Australia.
Dr F Mukhtar, PhD, School of Health Sciences, Universiti Sains Malaysia, Kelantan, Malaysia.
Address for correspondence: Dr Firdaus Mukhtar, School of Health Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia.
Tel: (60) 9766 3968; Fax: (60) 9764 7884; E-mail: firdaus@kb.usm.my
Submitted: 21 January 2008; Accepted: 18 April 2008
Abstract
Objective: To examine the factor structure of the Automatic Thoughts Questionnaire-Malay and report its validity and reliability in Malaysia.
Participants and Methods: One thousand and ninety patients from 4 different samples completed the Automatic Thoughts Questionnaire-Malay, as well as additional questionnaires which measured mood, cognition, and quality of life.
Results: Exploratory factor analysis revealed a 2-factor solution and accounted for 51% of the total variance, and a subsequent confirmatory factor analysis confirmed the 2-factor solution was acceptable for the data. The 2 factors appeared to describe negative self-concept / negative expectation and personal maladjustment The Cronbach's alpha coefficients ranged from 0.83 to 0.93. Evidence was also found to support the concurrent and discriminant validity of the Automatic Thoughts Questionnaire-Malay.
Conclusion: This report shows that the Automatic Thoughts Questionnaire-Malay is a reliable and valid instrument for measuring negative automatic thoughts in the Malay population.
Key words: Automatism; Depressive disorder; Factor analysis, statistical; Psychometrics
摘要
目的:研究自動思維問卷(馬來版)的因素結構,和報告這問卷在馬來西亞應用的效度和信度。
參與者與方法:1,090位來自四個不同組別的病人填寫自動思維問卷(馬來版) ,以及另外一些量度心情、認知和生活質素的問卷。
結果:探索性因素分析顯示有二因素模型,佔整體方差51% ,其後的驗證性因素分析顯示這二因素模型根據本研究的數據屬可接受。兩項因素描述負面自我概念/ 負面想法及個人調適不良。Cronbach's alpha系數介乎0.83與0.93之間。有證據支持自動思維問卷(馬來版)的同時效度及區辨效度。
結論:本研究顯示自動思維問卷(馬來版) 是量度馬來西亞人負面自動思維的一個可信及有效的工具。
關鍵詞:自發主義、抑鬱症、統計性因子分析、心理測量學
Cognitive behaviour therapy (CBT) focuses on altering negative cognitive structures to alleviate the symptoms of depression.1,2 In western populations, the Automatic Thoughts Questionnaire (ATQ) has been used in clinical settings for more than 20 years and is one of the most widely used cognitive measures for research on depressive cognition.3 Valid and reliable cognitive measures would improve the theoretical and empirical validity of the cognitive behavioural approach in Malaysia. Indeed, outcome studies of cognitive behavioural approaches have emphasised the consequences of maladaptive cognitive structures and negative self-statements.4,5 However, no studies have looked at the psychometric properties and factor structure of the ATQ in Malaysia, in particular for Malays.
The original version of the ATQ was found to have satisfactory reliability and validity among clinical and non- clinical samples.5 Additional studies have further supported the adequacy of the ATQ in terms of internal consistency and validity among students,3,6 psychiatric patients,4,6-8 the general community,9 and also among children.10 Since its establishment, the ATQ has been translated into a number of different languages, ranging from Persian,11 Norwegian,12 Turkish,13 and Chinese,14 testifying to its worldwide applicability.
The original study revealed that the ATQ possessed high internal consistency. Subsequent studies in Caucasian and non-Caucasian populations have reported parallel findings.3,6,10,11,13-15 A growing number of studies reported evidence of discriminant validity3,5,10 and concurrent validity.5,7,12 Positive relationships were found between the ATQ and a variety of depression instruments regardless of the sample (clinical or non-clinical). The ATQ has been found to correlate with the Beck Depression Inventory (BDI),3,11 the Minnesota Multiphasic Personality Inventory-Depression Scale,5 and the State-Trait Anxiety Inventory.5 The ATQ has demonstrated sensitivity to treatment effects.7,16
Studies investigating the psychometric properties of the ATQ produce mixed findings. A growing number of studies indicated that the ATQ is a reliable and valid instrument, while results pertaining to the factorial validity of the ATQ have been inconsistent. There are 4 dimensions in the original ATQ5 — personal maladjustment, negative self-concept and negative expectation, low self-esteem, and giving up / helplessness. Different factorial structures of the ATQ have been revealed in subsequent research. Two factors (negative self-concept / negative expectation, and personal maladjustment / desire to change) were revealed among undergraduate students,15 and only a single factor was revealed for the general community.9 Factorial validity inconsistency has also been revealed in Sahin and Sahin’s study,13 which found 5 factors of the ATQ (negative self-concept, confusion / escape fantasies, personal maladjustment and desire to change, loneliness / isolation, and giving up / helplessness) among a Turkish population. The study also found that none of the proposed factorial models fitted the data in Persians.11
Despite strong evidence of ATQ factorial validity in the western literature, support from non-western research remains inadequate. However, in Malaysia, research on the psychometric properties and factor structure of the ATQ had not been done. Further investigation is necessary to verify the validity of this instrument and thus ascertain the validity of the cognitive behavioural approach in Malaysia. In order to establish CBT as an effective approach in Malaysia, particularly for ethnic Malays, it is important to ensure that ATQ is a valid and reliable instrument as Malay attitudes and behaviour are strongly influenced by religion (Islam) and cultural traditions. Malays are greatly concerned about what other people think about them and are taught be intolerant of unlawful behaviour, such as premarital sex or the consumption of alcohol.17 Studies have reported that Malay patients commonly link mental illness with supernatural agents, a factor that may indirectly affect their attitudes to depression.18,19 Investigation of the psychometric properties of an instrument such as the ATQ in Malaysia, in a non- western cultural setting, might also extend our knowledge of its theoretical and empirical validity and provide further evidence for the universality of the construct.
It is therefore the intention of this paper to report on the psychometric properties and validity of the ATQ when used to assess Malays in Malaysia. Our aims were twofold; first, to investigate the ATQ-Malay factor structure and second, to establish its psychometric properties, specifically in a Malay cultural context.
Methods
Participants
A total of 1,090 participants were recruited for this study. The sample consisted of 315 (29%) students, 495 (45%) members of the general community, 167 (15%) patients from a primary care unit, and 113 (10%) patients diagnosed with major depressive disorders from a psychiatric clinic. Of the participants, 75% were women. The participant’s ages ranged from 18 to 63 years, with a mean of 26 years. The educational background of the participants included high school certificate level (48%), diploma / certificate level (17%), and university degree (33%); 1% of the participants had only completed primary school and 2% did not specify their level of education.
Measures
Automatic Thoughts Questionnaire
The 30 items of the ATQ5 measure the frequency of negative automatic thoughts. Respondents rated the frequency of the 30 negative thoughts on a 1-to-5 scale. For instance, how often negative automatic thoughts such as “I’m a loser” have occurred in the past week; higher scores indicate increased severity of negative thoughts. In a review study, the ATQ had high reliability, concurrent and discriminant validity, and strong sensitivity to treatment effects.20
Beck Depression Inventory–Malay
The BDI-Malay is a translated version of the original BDI21 with 20 items22 that provide an indication of the level of depressed mood. Participants responded to questions asking how they had felt over the past week, with higher scores indicating more severe depression. The BDI-Malay is divided into 2 subscales: cognitive / affective subscale and somatic / performance subscale. The full scale is considered to have strong psychometric properties among Malays in Malaysia.22
Dysfunctional Attitude Scale–Malay
The 19 items of the Dysfunctional Attitude Scale–Malay (DAS-Malay)23 is a translated version of the original DAS24 with 40 items that ask for 1 of 7 responses ranging from “totally agree” to “totally disagree”. This questionnaire measures the presence of more permanent dysfunctional attitudes to life, which predispose an individual to depression25; an example being, “If I fail at my work, then I am a failure as a person.” The scale has acceptable internal consistency and concurrent validity and was able to discriminate between depressed and non-depressed samples23; lower scores indicate less dysfunctional attitudes.
Zung Depression Self-Rating Scale–Malay
The Zung Depression Self-Rating Scale–Malay (Zung SDS- Malay) is a translated version of the original Zung SDS,26 which was designed for assessing depression in patients whose primary diagnosis was a depressive disorder. The 20 items address each of the 4 most commonly found character- istics of depression: its pervasive effect, its physiological equivalents, other disturbances, and psychomotor effects, such as “I have trouble sleeping at night” and “I have trouble with constipation”. Ten items are worded positively and 10 items are worded negatively. Each item is scored on a scale of 1 to 4 (“a little of the time” to “most of the time”) with reverse scaling for the negatively worded items. The total score ranges from 20 to 80, within which most people with depression score between 50 and 69, while a score of 70 and above indicates severe depression.26
World Health Organization Quality of Life Scale
The WHO Quality of Life (WHOQOL-BREF) version in Bahasa Malaysia (WHOQOL-BREF Malay)27 consisting of 26 items has been validated in Malaysia, with indications of good discriminant validity, construct validity, internal consistency (0.64 to 0.80), and test-retest reliability (0.49 to 0.88). The scale is a valid and reliable assessment of quality of life, especially for those with illness. Four domains extracted from the WHOQOL-BREF are physical and psychological health, social, and environmental.
Beck Hopelessness Scale–Malay
The Beck Hopelessness Scale–Malay (BHS-Malay) is a translated version of the original BHS28 with a 20-item scale for measuring negative attitudes about the future. The scale’s manual claims internal consistency ranging from 0.82 to 0.93 and a test-retest reliability of 0.6928; examples of questions asked are “My future seems dark to me” and “I can’t imagine what my life would be like in ten years”.
Procedure
Student Sample
A total of 315 undergraduates from 2 universities (studying medicine, dentistry, allied health sciences, and human sciences) participated voluntarily in this study to partially satisfy a research requirement of their course. All data were collected through group administrators. Each subject was provided with questionnaires as described above, with an explanation and accompanying directions for their use. A number of non-ethnically Malay students participated but their data were not included in the analysis to ensure that the conditions of this study were met.
General Community Sample
Members of the general public participated in this study by completing questionnaires randomly distributed in public places by research assistants, and returning these in envelopes supplied.
Medical Patients Sample
The Malay medical patients were recruited from primary care clinics; an obesity clinic; ear, nose and throat clinics; and community care clinics. They completed questionnaires distributed by research assistants and returned them in envelopes supplied. Participants were excluded if they were current drug or alcohol abusers, had a history of organically based cognitive dysfunction, demonstrated reading difficulties, were not fluent in Bahasa Malaysia, or were not ethnic Malays.
Patients with Major Depressive Disorders
Malay patients with depression were invited via mail, phone, or through referral from psychiatrists who had been informed of the study. A letter of invitation and information regarding the study was provided and those participants who were willing to participate presented at the psychiatric clinic for the intake procedure assessment. The second author, who works as a clinical psychologist, further evaluated the diagnosis of major depressive disorder using a structured clinical interview from the Diagnosis and Statistical Manual of Mental Disorder–4th Edition (DSM-IV) to ascertain participants’ eligibility. Participants were included if they were diagnosed as suffering from major depression or dysthymia as defined by the DSM-IV. Patients were excluded if their depression was secondary to another major psychiatric disorder (e.g. schizophrenia), if they were currently abusing drugs or alcohol, had a history of an organically based cognitive dysfunction, demonstrated reading difficulties, or were not fluent in Bahasa Malaysia.
Translating and Back-translating Procedure
Four bilingual psychologists with a Master’s degree or higher translated the Malay version of all the instruments (except WHOQOL-BREF) using back-translating procedures. A professional language interpreter was recruited to proofread the translated questionnaires to ensure their overall suitability and to resolve word ambiguity issues after translation. The back-translated versions were similar to the original versions and to each other. Minor differences concerning use of colloquial expressions in both languages were reconciled.
Ethical Approval
All participants gave their signed informed consent before undertaking the assessment. Ethical approval was sought from the research ethics committees belonging to the Ministry of Health of Malaysia and all the hospitals and institutions participating in this study.
Statistical Analyses
The Statistical Program for the Social Sciences (SPSS version 14.0, SPSS Inc., Chicago [IL], US) and AMOS version 6.0 (SPSS Inc., Chicago [IL], US) were used to analyse data in this study. A number of statistical procedures were used and descriptive statistics were used for data screening. Cronbach’s alpha coefficients (α) were computed to evaluate the reliability of the questionnaire, and correlations were calculated to examine the concurrent validity of the BDI, using the total sample. Discriminant analyses were used to evaluate the discriminant validity, specificity, and sensitivity of the BDI-Malay scores.
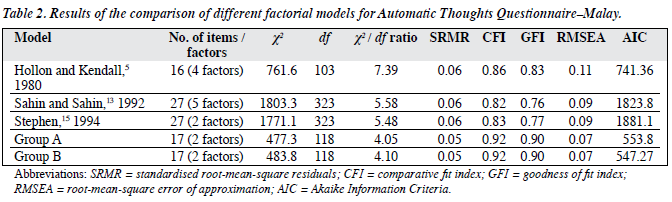
In this study the confirmatory factor analysis (CFA) model fit was evaluated using multiple fit indices.29 The indices selected were the Chi-square statistics (χ2), the comparative fit index (CFI),30 the standardised root-mean- square residuals (SRMR),31 the goodness of fit index (GFI), the root-mean-square error of approximation (RMSEA),32 and the Akaike Information Criteria (AIC).33 A good model fit is indicated by values of 0.90 or higher for the CFI and GFI. For the SRMR and RMSEA, values of 0.05 or lower indicate a close fit, while values less than 0.08 indicate an acceptable fit,32 and the one with the lowest AIC value is preferred in model comparisons.29
Results
Assumption Testing
Prior to conducting the primary analyses, the data were examined for accuracy, missing values, outliers and multivariate assumptions. The number of missing values was minimal (< 5%) and seemed to be distributed randomly across the remaining cases, therefore, mean substitution was employed where necessary. The Mahalanobis distance was used to identify multivariate outliers; using a cut-off of 0.001, no outliers were identified. The frequency distributions were further assessed using skewness and kurtosis statistics. Inspection of skewness and kurtosis indices indicated that departures from normality were not severe, so no variable transformations were deemed necessary.
Exploratory Factor Analysis: Group A
It was decided to divide the total sample (n = 1,090) into 2 groups, by using the odd-even split method (Group A [n = 545]; Group B [n = 545]). Group A was subjected to an exploratory factor analysis (EFA) to establish the factor structure and Group B was subjected to the CFA to confirm the ATQ-Malay factor structures found in Group A. Following Tabachnick and Fidell’s suggestion,34 a principal axis factoring with oblique rotation was employed in the initial exploratory analysis; upon examination of the correlation matrices, a substantial number of correlations greater than 0.33 were found, suggesting a favourable data set. Favourable values of the Kaiser-Meyer-Olkin value (0.95) and a significant value from Bartlett’s Test of Sphericity (p < 0.001) also suggested that the data were suitable for factor analysis. A number of criteria were used to check that the most appropriate number of factors to retain was consistent with previous studies15: (a) minimum eigenvalues of 1, (b) minimum factor loadings of 0.40, (c) minimal factorial complexity (multiple loading), and (d) meaningful interpretation of factors. The results indicated that 2 factors rotated to a simple structure using the Direct Oblimin method with Kaiser normalisation.
Using the above criteria, 2 factors were extracted. Item descriptions, factor loadings, and communality estimates are shown in Table 1. These two factors accounted for 51.0% of the variance in scores. Factor 1, which was labelled negative self-concept / negative expectation, accounted for 46.7% of the variance, while Factor 2 accounted for 4.28% of the variance. Factor 2 was subsequently labelled personal maladjustment.

Confirmatory Factor Analysis
Before the EFA results were presented, CFA models from western populations5,13,15 were tested for their goodness of fit with the data from the present study.
The Hollon and Kendall (1980) Model
The first model examined was Hollon and Kendall’s 4- factor model.5 The results of the fit indices were obtained (χ² = 761.68, df = 103, p < 0.001; CFI = 0.86; GFI = 0.83; SRMR = 0.06; RMSEA = 0.11), so the model provided a poor fit to the data as judged by all fit indices (Table 2). These analyses showed that Hollon and Kendall’s 4-orthogonal factor model with 16 items did not fit well with our data set.
The Sahin and Sahin (1992) Model
Table 2 also shows results for the fit indices of the second model tested, Sahin and Sahin’s13 5-orthogonal factor model. Results of fit indices were obtained (χ² = 1803.3, df = 323, p < 0.001; CFI = 0.82; GFI = 0.76; SRMR = 0.06; RMSEA = 0.09), so this model provided a poor fit with the data as judged by all fit indices. The analyses showed that Sahin and Sahin’s 5-factor model with 27 items again was not a good fit with the data.
The Stephen (1994) Model
The third model tested was Stephen’s15 2-correlated factor model. Results of fit indices were obtained (χ² = 1771.1, df = 323, p < 0.001; CFI = 0.83; GFI = 0.77; SRMR = 0.06; RMSEA = 0.09), so this model provided a poor fit to data (Tables 1 and 2). The analyses showed that Stephen’s 2- factor model with 27 items did not fit well with the data.
Preliminary Confirmatory Factor Analysis with Group A
Confirmatory factor analysis was subsequently applied to Group A data to examine the construct validity of the 2- correlated factor model extracted from the EFA. Initially, 25 predictors (items) were used to test the model but most of the fit indices suggested an inadequate fit (χ² = 1382.3, df = 274, p < 0.001; CFI = 0.87; SRMR = 0.05; RMSEA = 0.09). Given these results, it was decided that the model required further specification. Inspection of the squared multiple correlation (R2) suggested that the number of specified latent factors was the potential source of the problem. Specifically, a substantial number of R2 values of less than 0.5 were found, casting doubt on the extent to which these items contributed to the factor they were designed to measure.31 Further inspection of the standardised residuals covariance revealed several pairs of items with large residuals (> 2.38). Deletion of these items (items 17, 18, 24, 23, 28, 10, 8, 26) resulted in an improved model fit.
Final Confirmatory Factor Analysis with Group A
In a subsequent analysis, based on modified indices results, 17 items were included in the final CFA to test the fit of the model (Table 2). Using maximum likelihood procedures to estimate the model, the results indicated that reasonable fit indices were obtained (χ² = 477.3, df = 118, p < 0.001; CFI = 0.92; GFI = 0.90; SRMR = 0.05; RMSEA = 0.07). The Figure demonstrates standardised regression weight for items in the ATQ-Malay.
Confirmatory Factor Analysis with Group B
The 2-factor model was further evaluated using an independent (Group B) validation sample (n = 545). Results of the CFA for Group B are also displayed in Table 2. Using maximum likelihood estimation procedures, excellent fit indices were obtained (χ2 = 483.8, df = 118, p < 0.001; CFI = 0.92; GFI = 0.90; SRMR = 0.05; RMSEA = 0.07), suggesting the stability of its factor structure. These findings confirmed the CFA results from Group A and suggested that the factor structure for the ATQ-Malay is valid and stable.
Reliability and Validity of the Automatic Thoughts Questionnaire–Malay
Internal Consistency
The whole sample (n = 1,090) was used to calculate the reliability and validity of the ATQ-Malay. Table 1 shows how the reliability of the 2 latent factors (17 items of the ATQ-Malay) was evaluated. Using Cronbach’s alpha to estimate the reliability coefficient, a good alpha value was obtained for the overall scale (0.93) and the subscales (negative self-concept / negative expectation = 0.91; personal maladjustment = 0.83).
Concurrent Validity
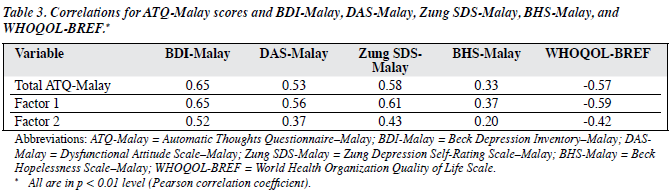
Both concurrent factors were evaluated using the Pearson correlation coefficient. Descriptions of the scales and their intercorrelations are shown in Table 3. Evidence of concurrent validity was revealed by a significantly positive correlation between the ATQ-Malay total scores and the BDI-Malay (r = 0.65), the DAS-Malay (r = 0.53), Zung SDS-Malay (r = 0.58), BHS-Malay (r = 0.33), and negative correlation with the WHOQOL-BREF (r = –0.57). Furthermore, the results also reveal a significantly positive correlation between negative self-concept / self-expectation and the BDI-Malay (r = 0.65) and Zung SDS-Malay (r = 0.61), the DAS-Malay (r = 0.56), BHS-Malay (r = 0.37), and significantly negative relationship with WHOQOL- BREF (r = –0.59). The final subscale of the ATQ-Malay and personal maladjustment showed a moderately significant relationship for both symptom measures (BDI-Malay, r = 0.52; Zung SDS-Malay, r = 0.43), the WHOQOL-BREF (r = –0.42), the DAS-Malay (r = 0.37), and BHS-Malay (r = 0.20). This demonstrates that the ATQ-Malay has moderate concurrent validity.
Discriminant Validity
A direct discriminant analysis using all 17 items of the ATQ-Malay was performed. Table 4 shows that the clinical group (patients with depression) demonstrated significantly higher mean scores on the ATQ-Malay than subjects in the 3 non-clinical groups (students, the general community, and general medical patients). A classification sub-analysis used a linear combination of all 17 items. As an indicator of sensitivity, the analysis indicated that high total scores from the ATQ-Malay detected 36.3% of the patients with depression (Table 5). Meanwhile, the specificity analysis found that 2.8% of the non-clinical subjects had high levels of negative automatic thoughts. It was found that 97.2% of subjects in the non-clinical group (n = 977) and 63.7% of subjects in the clinical group (n = 113) had low ATQ-Malay scores. The overall percentage of correctly classified cases was 90.9%.

Table 5 reports the negative self-concept / negative expectation factor. The analysis indicated that this factor was able to detect 38.9% of clinical subjects and 3.7% of the non-clinical subjects who reported high scores in negative self-concept / negative expectation. Meanwhile, 96.3% of the non-clinical group and 61.1% of the clinical group reported low scores for this factor. The overall percentage of correctly classified cases was 90.4%. The personal maladjustment factor is shown in Table 5. The analysis indicated that this factor was able to detect only 5.3% of the clinical subjects and 1.0% of the non-clinical subjects reporting high scores in personal maladjustment. The overall percentage of correctly classified cases was 89.3%. These results suggest that the ATQ-Malay items are able to discriminate between clinical and non-clinical subjects.

Discussion
This study aimed to assess the psychometric properties of the ATQ-Malay among Malays in Malaysia and our results suggest the factor structures are different from research conducted in other non-western populations. We have found that the EFA was comprised of 2 related factors, one reflecting negative self-concept / negative expectation while the other indicated personal maladjustment. This result is consistent with a study by Stephen15 in which a 2-factor solution was obtained for the ATQ. Six items (items 11, 21, 12, 6, 30, and 29) from this study are similar to Stephen’s factor 1 (negative self-concept and negative expectation). Four items (items 20, 14, 3, and 2) from this study are similar to Hollon and Kendall’s5 factor 2 (personal maladjustment and desire to change). Both Hollon and Kendall5 and Stephen15 did not find a significant loading for item 13 (“I cannot get started”). In the present study, the item is loaded on factor 1 (negative self-concept and negative expectation) and was found to be significant in Sahin and Sahin’s study,13 but they labelled it independently as confusion and escape fantasy.
It should be noted that in the EFA analysis, the 5 items that did not have significant loadings (> 0.40) were discarded. These were items 15, 9, 8, 7, and 1. Initially, an exploratory CFA analysis found that the model did not have a good fit with the data. Consequently, 8 items were discarded due to a large standardised residuals covariance (> 2.58), and the GFI gradually improved. In the final model, 17 items were retained for further validation analysis with Group B. Most of the previous studies in the West5,15 have reported a significant loading of items 7 and 26 on a ‘desire to change’ factor. These items were not significant when measuring negative automatic thoughts among Malays who follow Islam. This is probably due to Islamic teachings implying that a desire to change is necessary for everyone and is not associated with depression. Islam defines a person or insan (an Arabic term) as a weak, imperfect, and forgetful human being who needs to rely upon and have faith in a superior being (Allah).35 This is to ensure that Muslims follow the right path during their earthly lives and also during life after death. This may be affected by the notion that God (Allah) will not change a person’s living conditions until they put in an effort to improve themselves.36 The idea that wishing to be a better person would be judged as negative thinking or associated with depression seems inappropriate to Muslims.
It is interesting to note that the final model of CFA results from Group A and the cross-validation from Group B data showed that the 17 items and 2 factors of the ATQ- Malay had a reasonably good fit. The ATQ-Malay proved to have sufficient internal consistency and reliability. Although Cronbach’s alpha coefficients obtained in this study were somewhat lower than those obtained in the original study,5 they were higher than those found by Dobson and Breiter3 but inconsistent with the French and Turkish versions of the ATQ (0.93).13 The negative self-concept and negative expectation, however, showed an excellent reliability coefficient (0.91), while the personal maladjustment yielded satisfactory reliability (0.83). The present study further verified the concurrent validity of the ATQ-Malay. Previous studies have also supported the positive relationship between the ATQ and the BDI.5,11-14 Our findings also showed that the ATQ-Malay scores had good sensitivity and specificity for discriminating between clinical and non-clinical samples.4,6
This is one of the first studies to validate the ATQ-Malay for use in large and diverse populations and to subject 2 subscales to factor analysis. There is evidence that the ATQ-Malay is sufficiently reliable and valid for measuring negative thoughts in depression. The major strength of the present study was the use of a large sample (n = 1,090), the use of EFA and CFA methodology, and the direct application of a theoretically derived measure in a clinical setting and a specific sample. The robustness of this study is further supported by the cross-validation of the CFA model in a different group of participants.
Though the structures of schemas that predispose individuals to depression may have been acquired through different pathways in different socio-cultural contexts, the final depressed state, in terms of self-related automatic negative thoughts, may have generality across cultures. In conclusion, the findings show that the ATQ-Malay has good psychometric properties and is a reliable instrument for capturing automatic negative thoughts in a Malay cultural context.
References
- Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. New York: Guilford; 1979.
- Oei TP, Bullbeck K, Campbell JM. Cognitive change process during cognitive behaviour therapy for depression. J Affect Disord 2006;92:231-41.
- Dobson KS, Breiter HJ. Cognitive assessment of depression: reliability and validity of three measures. J Abnorm Psychol 1983;92:107-9.
- Harrel TH, Ryon NB. Cognitive-behavioral assessment of depression: clinical validation of the automatic thoughts questionnaire. J Consult Clin Psychol 1983;51:721-5.
- Hollon SD, Kendall PC. Cognitive self-statements in depression: Development of an automatic thoughts questionnaire. Cognit Ther Res 1980;4:383-95.
- Hill CV, Oei TP, Hill MA. An empirical investigation of the specificity and sensitivity of the Automatic Thoughts Questionnaire and Dysfunctional Attitudes Scale. J Psychopathol Behav Assess 1989;11:291-311.
- Clark DA. The validity of measures of cognition: A review of literature. Cognit Ther Res 1988;12:1-20.
- Hollon SD, Kendall PC, Lumry A. Specificity of depressotypic cognitions in clinical depression. J Abnorm Psychol 1986;95:52-9.
- Netemeyer RG, Williamson DA, Burton S, Biswas D, Jindal S, Landreth S, et al. Psychometric properties of shortened versions of the Automatic Thoughts Questionnaire. Educ Psychol Meas 2002;62:111-29.
- Kazdin AE. Evaluation of the Automatic Thoughts Questionnaire: Negative cognitive processes and depression among children. Psychol Assess 1990;2:73-9.
- Ghassemzadeh H, Mojtabai R, Karamghadiri N, Ebrahimkhani N. Psychometric properties of a Persian-Language version of the Automatic Thoughts Questionnaire: ATQ-Persian. Int J Soc Psychiatry 2006;52:127-37.
- Chioqueta AP, Stiles TC. Norwegian version of the automatic thoughts questionnaire: a reliability and validity study. Cogn Behav Ther 2004;33:79-82.
- Sahin NH, Sahin N. Reliability and validity of the Turkish version of the Automatic Thoughts Questionnaire. J Clin Psychol 1992;48:334- 40.
- Cao R, Chen S, Tang W, Song H. The reliability and validity of the Automatic Thoughts Questionnaire. Chin J Clin Psychol 2001;9:108-9.
- Stephen J. Subscales of the Automatic Thoughts Questionnaire. J Genet Psychol 1994;155:367-8.
- Simons AD, Garfield SL, Murphy GE. The process of change in cognitive therapy and pharmacotherapy for depression. Changes in mood and cognition. Arch Gen Psychiatry 1984;41:45-51.
- Mastor KA, Jin P, Cooper M. Malay culture and personality: A Big- Five. Am Behav Sci 2000;44:95-111.
- Razali SM, Khan UA, Hasanah CI. Belief in supernatural causes of mental illness among Malay patients: impact on treatment. Acta Psychiatr Scand 1996;94:229-33.
- Razali SM, Najib MA. Help-seeking pathways among Malay psychiatric patients. Int J Soc Psychiatry 2000;46:281-9.
- Glass CR, Arnkoff DB. Questionnaire methods of cognitive self- statement assessment. J Consult Clin Psychol 1997;65:911-27.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:53-63.
- Mukhtar F, Oei TPS. Exploratory and confirmatory factor analysis and psychometric properties of Beck Depression Inventory-Malay (BDI-Malay) in Malaysia. Proceedings of the Transcultural Psychiatry Conference; 2007 Apr 27-29; Japan.
- Mukhtar F, Oei TPS. Exploratory and confirmatory factor validation and psychometric properties of the Dysfunctional Attitude Scale in Malaysia. Proceedings of the 10th Johore Mental Health Convention; 2008 Jul 10-13; Malaysia.
- Weissman AN, Beck AT. Development and validation of the Dysfunctional Attitude Scale: A preliminary investigation. Proceedings of the Annual Meeting of the American Educational Research Association; 1978 Nov; Toronto, Canada.
- Clark DA, Beck AT, Alford BA. Scientific foundations of cognitive theory and therapy of depression. Hoboken, NJ, US: John Wiley & Sons Inc.; 1995.
- Zung WW. A self-rating depression scale. Arch Gen Psychiatry 1965;12:63-70.
- Hasanah CI, Naing L, Rahman AR. World Health Organization Quality of Life Assessment: brief version in Bahasa Malaysia. Med J Malaysia 2003;58:79-88.
- Beck AT, Steer RA. Beck Hopelessness Scale. San Antiano, TX: Psychological Corp; 1988.
- Kline RB. Principles and practice of structural equation modeling. New York: The Guildford Press; 1998.
- Bentler PM. Comparative fit indexes in structural models. Psychol Bull 1990;107:238-46.
- Hu LT, Bentler PM. Evaluating model fit. In: RH Hoyle, editor. Structural equation modeling, Thousand Oaks, CA: Sage; 1995.
- Browne MW, Cudeck R. Alternative ways of assessing model fit. Sociol Methods Res 1993;21:230-58.
- Akaike H. Factor analysis and AIC. Psychometrika 1987;52:317-22.
- Tabachnick BG, Fidell LS. Using multivariate statistics. Boston: Allyn and Bacon; 2000.
- Latino American Dawah Organization. Islamic resources for beginners. Available from: http://www.latinodawah.org. Accessed 14 Jan 2007.
- International Islamic University Malaysia. Ali Y. The Holy Book: translation. Available from: http://www.iiu.edu.my/deed/quran/malay. Accessed 14 Jan 2007.
