
Hong Kong J Psychiatry 2005;15(1):14-17
ORIGINAL ARTICLE
JCW Leung, VWC Lui, LCW Lam
Dr Jimmy CW Leung, MB ChB, Department of Psychiatry, Tai Po Hospital, The Chinese University of Hong Kong, Tai Po, Hong Kong, China.
Dr Victor WC Lui, MBBS, MRCPsych, FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, Tai Po Hospital, The Chinese University of Hong Kong, Tai Po, Hong Kong, China.
Dr Linda CW Lam, MB ChB, MRCPsych, FHKCPsych, FHKAM (Psychiatry), Department of Psychiatry, Tai Po Hospital, The Chinese University of Hong Kong, Tai Po, Hong Kong, China.
Address for correspondence: Dr Linda CW Lam, Department of
Psychiatry, G/F, Multi-centre, Tai Po Hospital, Tai Po, Hong Kong, China.
Tel: (852) 2607 6026; Fax: (852) 2667 1255;
E-mail: cwlam@cuhk.edu.hk
Submitted: 6 July 2004; Accepted: 17 May 2005
Abstract
Objective: Alzheimer's disease is an increasing problem among the Chinese population. Earlier intervention will reduce the burden of the disease for patients, their families, and society. In this study, the usefulness of the Clock Drawing Test for screening for early Alzheimer's disease was examined.
Patients and Methods: The Clock Drawing Test and Clock Copying Test were administered to 66 elderly Chinese patients with early Alzheimer's disease and 66 age-matched, community- dwelling, elderly Chinese people without dementia for comparison. The Chinese Clock Draw- ing Test scoring criteria were used.
Results: Significant differences in Clock Drawing Test scores were found between patients with Alzheimer's disease and controls (p < 0.001). Clock Drawing Test performances were significantly correlated with educational level in both groups. Optimal cut-off points for participants for different educational levels were identified. The sensitivities of the Clock Drawing Test for screening for early Alzheimer's disease among participants with minimal (<2 years) and elementary (2 to 6 years) education were 72.8% and 75.0%, respectively. Positive predictive values obtained by combining the Clock Drawing Test and Clock Copying Test were 73.9% and 95.2% for participants with minimal and elementary education, respectively.
Conclusions: The Clock Drawing Test is a useful tool for screening for early Alzheimer's dis- ease among the elderly Chinese population with elementary educational level. The potential usefulness for differentiating dementia subtypes, particularly in combination with other screen- ing tools, should be further explored.
Key words: Alzheimer disease, Diagnosis
Introduction
Traditionally, the Clock Drawing Test (CDT) has been used to reflect parietal lobe function and to examine for visuo- spatial inattention.1,2 Although clock drawing is most often thought of as constructional in nature, the ability to draw an intact clock face is a complex task requiring the integrity of different cognitive domains.3 The CDT is a potential measure of global cognitive function for epidemiological studies because it is easy and quick to administer, and is relatively unaffected by language, cultural, or ethnic factors. The test can be reliably rated both by clinicians and trained observers, and generally has good inter-rater and test-retest reliability. The CDT also provides objective and graphic documentation of cognitive deficits that can be shared by the clinician with patients and family members.4-8
Studies have been performed to investigate the effec- tiveness of the CDT for recognising the early stage of dementia. Although the CDT is well known as a screening test for cognitive impairment and dementia, assessment of its validity for early diagnosis of the disorder is limited.5,9-13 In this study, we explored the potential use of the CDT and Clock Copying Test (CCT) for screening for early Alzheimer's disease (AD) in the elderly Chinese population, among which a relatively low literacy level is expected. To explore the effect of educational level on the performance of the CDT and CCT, patients were divided into 3 groups according to their educational level, and the applicability of the CDT for each group was studied.
Patients and Methods
Patients
Two groups of elderly Chinese people who had participated in a project to examine the behavioural and psychological symptoms of AD were recruited from October 2000 to June 2002. The first group comprised 66 patients with early AD (Clinical Dementia Rating [CDR], 114) who first presented to the psychogeriatric clinics at hospitals in the New Territories East region of Hong Kong. Sixty six cognitively intact, age-matched elderly people (CDR, 0) were recruited from local elderly social centres for comparison. Patients with profound sensory deficits or history of significant head injury or neurological disorder were excluded. The diagnosis of AD was evaluated by psychogeriatricians using the National Institute of the Neurological and Communicative Disorders and Stroke — Alzheimer's Disease and Related Disorders Association criteria.15 Severity of dementia was assessed by the same psychiatrist using the CDR. Patients with AD recruited for this study had early dementia and the controls were cognitively intact. Written consent was obtained from the patients or from first-degree relatives. The study was approved by the Ethics Committee of The Chinese University of Hong Kong.
Assessment
All participants were administered the Cantonese version of the Mini-Mental State Examination (CMMSE)16 and the CDT, which consists of 2 parts. In the first part, participants were asked to draw the numbers of a clock face with the hands indicating the 3-o'clock position inside a pre-drawn circle of 2.5 inches in diameter. The instruction was repeated if a participant did not understand the request. There was no time limit for completion of the drawing task. The second part comprised the CCT, in which participants were requested to read a pre-drawn clock face with the hands indicating 10 minutes to 3 o'clock. Participants were then requested to copy the clock face on a pre-drawn circle on the same sheet of paper. The Chinese CDT (CCDT) scoring criteria6 were used. A combined qualitative and quantitative approach was adopted for this scoring system. The preservation of time concept and integrity of constructional abilities were the major functions assessed. The score ranged from 0 to 10 and a high score denoted poor performance. The CDT was also evaluated by an independent scoring criterion devised by Shulman et al17 for comparison.
Statistical Analysis
The validity of the CCDT for screening of AD was estimated. CDT and CCT scores were compared between the patient and control groups using t tests. Concurrent validity was estimated by comparing the clock tests and CMMSE scores using correlation analysis. Reliability was evaluated by comparing the CDT scores with the Shulman clock test scores. Significance was set at p = 0.05. Sensitivity and specificity at different cut-off points were calculated to obtain the optimal value for screening for AD. Positive predictive values were estimated from a combination of optimal cut-off points in the CDT and CCT. The results were analysed using the Statistical Package for the Social Sciences version 10.0.
Results
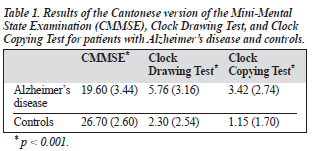
The mean age was 75.20 years (SD, 7.15 years; range, 51 to 90 years) for patients with AD and 74.9 years (SD, 4.64 years; range, 68 to 87 years) for the control group. The mean educational level was 3.94 years (SD, 3.85 years) for patients with AD and 4.47 years (SD, 4.97 years) for the control group. The mean (SD) CMMSE and CDT scores are shown in Table 1. Significant differences in CMMSE (t = 13.37; p < 0.001), CDT scores (t = -6.93; p < 0.001) and CCT scores (t = -5.72; p < 0.001) were found between the patients with AD and the control group. Correlations between the CDT and Shulman's scoring systems were calculated, and high agreement between the 2 scoring systems were identified (correlation coefficient = 0.97, p < 0.001).
CDT scores correlated significantly with age, educational level, and CMMSE scores for both groups (Pearson's cor- relation, p < 0.05). The correlations were less significant, particularly the CCT scores, for the patients with AD (Table 2).

Screening for Early Alzheimer's Disease
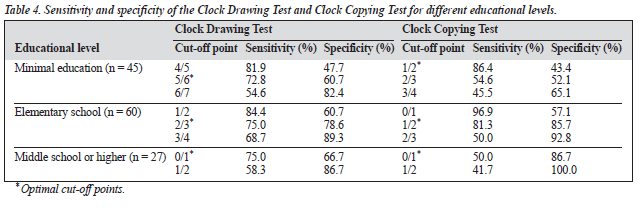
The CDT and CCT scores were compared with the clinical diagnosis of AD. At optimal cut-off points, the sensitivity and specificity of the CDT for screening for early AD were 78.8% and 63.6%, respectively, whereas the sensitivity and specificity of the CCT were 75.8% and 74.2%, respectively (Table 3). To explore the effect of educational level on the performance of the CDT and CCT, the sensitivity and speci- ficity for screening for early dementia were calculated with reference to 3 different educational levels: minimal education (<2 years, n = 45), elementary level (2 to 6 years, n = 60), and middle school or higher level (>6 years, n = 27) [Table 4]. The sensitivities of the CDT for screening for early AD among participants with minimal (<2 years) and elementary (2 to 6 years) education were 72.8% and 75.0%, respectively. The positive predictive values obtained by combining the CDT and CCT scores at the respective optimal cut-off points were 73.9% for the minimal educa- tion group, 95.2% for the elementary education group, and 89.4% for higher education group.

Discussion
This study examined the applicability of the CDT and CCT as screening tools for early AD in the elderly Chinese population. The significant correlation with CMMSE scores, and satisfactory sensitivity and specificity of the CCDT suggested that the CCDT scoring system is useful for screening for early AD in the elderly Chinese population in Hong Kong. The study also found a significant correlation between age and CDT scores in the control group. This was consistent with findings from previous studies involving neurologically healthy participants, that have reported that the proportion of errors in clock drawing increased with age.18,19 Previous studies have documented that clock drawing performance is highly correlated with educational level.2-4,20,21 Similar results were noted among the elderly Chinese population in this study. Among the different screening demographic variables, only educational level significantly correlated with CDT and CCT scores in both groups. The correlations between age and CMMSE scores with CDT scores were highly significant in the control group. It is possible that, in normal ageing, different demographic factors influ- ence the performance of clock drawing. For patients with a neurodegenerative disorder such as AD, the ability to draw a clock face is affected by the disease process and educational attainment may become a protective factor.
To determine the significance of education in the CDT and CCT, the educational levels were stratified when calcu- lating the sensitivities and specificities of the CDT when screening for early AD. The findings suggested that the optimal cut-off points of both tests were higher for patients with minimal education. For patients with the highest educa- tional level, the low cut-off points suggest that the useful- ness of CDT for the early detection of AD is limited. The task may be too simple for patients with a level of education higher than elementary level, even though the dementia process has started. A larger study of patients with early AD with high levels of education may help to further clarify whether clock face tests are applicable as a screening tool.
The CDT attained a relatively high sensitivity, but lower specificity, for detecting early AD in patients with minimal education. This result may be explained by the possibility that, for some elderly people with no formal education, the task of holding a pen to draw a clock face is not easy for them. As the main indication for using a screening tool for dementia is to identify potential patients for further assess- ment and follow up, the high sensitivity, albeit with lower specificity, still suggests that the CDT is clinically valid for patients with minimal education. Better sensitivity and speci- ficity were obtained for patients with an elementary educa- tional level. The CDT and CCT achieved a sensitivity and specificity of 75.0% and 81.3%, respectively, for detecting the early stage of dementia in this group of patients. It is likely that the acquisition of basic literacy has made the drawing of a clock face relatively simple for the control group, although the elementary educational level does not protect against deterioration of performance for patients with AD. While some studies suggested that the use of the CDT for the detection of early dementia is limited,9,13 the results of this study suggest a potential role in screening for early AD in the Chinese population, especially for people with an elementary educational level.
The CCT is a less useful tool for screening for AD when used alone. However, when the CDT and CCT scores were combined, the positive predictive values reached 73.9% and 95.2% for patients with minimal and elementary education, respectively. Previous studies have suggested that the differences in CDT and CCT scores may be representa- tive of executive function performance. Dementia syndromes of different aetiologies and differently affected executive functions may be differentiated by the variation between CDT and CCT scores. In this study, the analysis of dementia sub- types could not be evaluated using the CDT because only patients with AD were recruited.
Unlike other tools used for screening of cognitive function, CDT is independent of ethnic and cultural bias, which makes it user-friendly. Moreover, routine measures of cognition such as the MMSE often fail to identify execu- tive dysfunction, which often precedes the memory decline in early dementia in some patients. It has been documented that CDT is a moderately sensitive and specific test for de- tecting these changes compared with the MMSE.22 As well as being used alone, the CDT may also be combined with other quick tests as a short neuropsychological examination. The sensitivity and specificity have been noted to be greater than 90% in some studies.23
The CDT is a useful tool for quick screening for early AD in the elderly Chinese population. The test has satisfac- tory sensitivity and specificity, particularly for patients with elementary educational level.
Acknowledgements
We would like to thank Ms Candace Chan, Mr Edward Mok, and Mr TK Choy for their assistance in data collection. This work was supported by a grant from the Earmarked Research Grants Scheme of the Hong Kong Research Grants Council (CUHK 4082/00M).
References
- Battersby WS, Bender MB, Pollack M, Kahn RL. Unilateral 'spatial
- agnosia' ('inattention') in patients with cerebral lesions. Brain 1956; 79:68-93.
- Goodglass H, Kaplan E. Assessment of aphasia and related disorders. Philadelphia: Lea and Febiger; 1983.
- Tuokko H, Hadjistaropoulos T, Miller JA, Beattie BL. The clock-test: a sensitive measure to differentiate normal elderly from those with Alzheimer's disease. J Am Geriatr Soc 1992;40:579-584.
- Borson S, Brush M, Gil E, et al. The Clock Drawing Test: utility for dementia in multiethnic elders. J Gerontol A Biol Sci Med Sci 1999;54:M534-M540.
- Concepcion ES, Rungnirand P, Hideki U, David SG. Clock Drawing
- Test in very mild Alzheimer's disease. J Am Geriatr Soc 1998;46: 1266-1269.
- Lam LC, Fung HF, Ng KO, et al. Clock-face drawing, reading and setting tests in the screening of dementia in Chinese elderly adults. J Gerontol B Psychol Sci 1998;53:353-357.
- Shulman K. Clock-drawing. Is it the ideal cognitive screening test? Int J Geriatr Psychiatry 2000;15:548-561.
- Sunderland T, Hill JL, Mellow AM, et al. Clock drawing in Alzheimer's disease — a novel measure of dementia severity. J Am Geriatr Soc 1989;37:725-729.
- Lee H, Swanwick GR, Coen RF, Lawler BA. Use of the clock drawing task in the diagnosis of mild and very mild Alzheimer's disease. Int Psychogeriatr 1996;8:469-476.
- Powlishta KK, Von Dras DD, Stanford A, et al. The clock drawing test is a poor screen for very mild dementia. Neurology 2002;59:898-903. Moretti R, Torre P, Antonello RM, Cazzato G, Bava A. Ten-Point Clock Test: a correlation analysis with other neuropsychological tests in dementia. Int J Geriatr Psychiatry 2002;17:347-353.
- Yasuko F, Hajime T, Tomoko A, Toru K. Development of a short neuro- psychological battery to screen early dementia in the elderly. Geriatr Gerontol Int 2002;2:179-186.
- Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia: Br J Psychiatry 1982;140: 556-572.
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer's disease: report of the NINCDS- ADRDA work group under the auspices of Department of Health and Human Services task force in Alzheimer's disease. Neurology 1984; 34:939-944.
- Chiu HF, Lee HC, Chung WS, Kwong PK. Reliability and validity of the Cantonese version of the Mini-Mental State Examination — a preliminary study. J Hong Kong Coll Psychiatrists 1994;4 (Suppl 2): 25-28.
- Shulman KI, Gold DP, Carole A, Cohen Carla AZ. Clock-drawing and dementia in the community: a longitudinal study, Int J Geriatr Psychiatry 1993;8:487-496.
- Freedman M, Leach L, Kaplan E, Winocur G, Shulman K, Delis DC. Clock drawing: a neuropsychological analysis. New York: Oxford University Press; 1994.
- Paganini-Hill A, Clark LJ, Henderson VW, Birge SJ. Clock drawing: analysis in a retirement community. J Am Geriatr Soc 2001;49: 941-947.
- Ainslie NK, Murden RA. Effect of education on the clock-drawing dementia screen in non-demented elderly persons. J Am Geriatr Soc 1993;41:249-252.
- Lieberman D, Galinsky D, Fried V, et al. Factors affecting the results of the clock drawing test in elderly patients hospitalized for physical rehabilitation. Int J Geriatr Psychiatry 1999;14:325-330.
- Juby A, Tench S, Baker V. The value of clock drawing in identifying executive cognitive dysfunction in people with a normal Mini-Mental State Examination score. CMAJ 2002;167:859-864.
- Funabiki Y, Takechi H, Akamatsu T, Kita T. Development of a short neuropsychological battery to screen early dementia in the elderly. Geriatr Gerontol Int 2002;2:179-186.
