
Hong Kong J Psychiatry 2005;15(1):29-31
COMMENTARY
PSF Yip
Address for correspondence: Dr Paul SF Yip, Hong Kong Jockey Club Centre for Suicide Research and Prevention, Faculty of Social Sciences, The University of Hong Kong, Pokfulam, Hong Kong, China.
Tel: (852) 2241 5013; Fax: (852) 2549 7161;
E-mail: sfpyip@hkucc.hku.hk
Introduction
Suicide has become a public health concern worldwide. According to the World Health Organization (WHO), an estimated 1 million people died from suicides in 2000 — in other words, 1 suicide occurred every 40 seconds.1 In 2001, the global death toll from suicide far exceeded the number of deaths by homicide (500,000) and war (230,000).2 Sui- cide is also a particularly serious problem in the Western Pacific region: this region alone accounts for 38% of the world's suicides.1
In Hong Kong, too, suicides have cost our community dearly. According to the Hong Kong Jockey Club (HKJC) Centre for Suicide Research and Prevention,3 the total num- ber of suicide deaths reached 1264 in 2003 — equivalent to 18.6 per 100,000, which is 28% higher than the world average of 14.5 per 100,000. Moreover, suicide is the lead- ing cause of death among the 15- to 24-year age group, and the rate has surged by more than 70% since 1997. The estimated loss of labour productivity of suicide in 2003 was HK$1.4 billion. In addition, the number of suicides over- took the number of 'natural' deaths from infectious and parasitic diseases (1047); endocrine, nutritional and meta- bolic diseases (885); and traffic accidents (175) in 2003.3
A Public Health Approach to Suicide Prevention
The burden of suicide to our community can no longer be ignored. Unfortunately, the majority of the suicidal people are reluctant to seek help from health care professionals,3 probably because of the stigma towards treatment and uncertainty about treatment effectiveness. Suicide has traditionally been viewed as a mental health issue that is addressed primarily through clinical intervention, especially the treatment of depression.4 Nevertheless, it is also well known that approximately two-thirds of all people who com- mitted suicide did not receive any specialist psychiatric care in the year before death.5
On the basis of rigorous calculations, Lewis et al showed that high-risk strategies would have only a modest effect on population suicide rates, even if effective interventions were developed, and that the UK government's target for suicide reduction was more likely to be achieved using population- based strategies that aimed at actively reducing risk among the whole population.6 Furthermore, all research has pointed out that suicide can be the tragic endpoint of an interplay of a wide array of factors, including biological, genetic, social, cultural, psychological, and behavioural factors.7 For these reasons, it is imperative that multiple avenues be taken for sui- cide prevention and intervention. As the eminent psychiatrist Keith Hawton, from the Centre for Suicide Research at the University of Oxford, UK, put it, "Suicide rates are unlikely to decline as long as we confine our prevention efforts only to those who are at immediate risk of attempting suicide."
Flooding is a useful metaphor for the problem of suicide. When a flood occurs, rescue teams work hard to save those affected, focusing attention mainly on the victims who are swept downstream. However, the cause of the flood, includ- ing upstream conditions such as deforestation, are seldom dealt with or considered. What lies 'upstream' of the in- creasing number of suicides is often a malfunctioning society. A public health approach to suicide prevention has therefore been widely advocated by governments, inter- national organisations, and professional bodies worldwide (e.g., the USA Department of Health and Human Services, the WHO, and the International Association of Suicide Prevention).2,8,9 This approach acknowledges the importance of both the high-risk and the population-based strategies to suicide prevention, and requires a multi-sector effort to tackle the problem at multiple levels: in the community (universal strategies), among specific population subgroups (selective strategies), and among those at a particularly high risk of suicidal behaviour (indicated strategies) [Table 1].10

All 3 strategies represent subtypes of primary prevention. More conventional forms of treatment, such as health status maintenance and aftercare (including rehabilitation), may be distinguished from these 3 types of primary prevention. Altogether, these measures form a spectrum of health care intervention.11
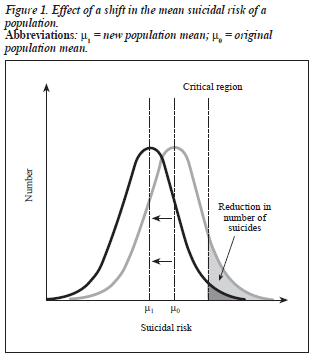
By virtue of its systematic approach to prevent illness, disability, and premature death, the public health strategy provides a strong framework for creating an effective, con- certed effort to prevent suicide. In other words, public health intervention not only tackles the 'downstream' problems, but also aims at improving the 'upstream' conditions. The Rose Theorem states that a large number of people exposed to a low risk may generate more cases than a small number exposed to a high risk.12 The proverb "an ounce of preven- tion is better than a pound of cure" echoes the idea behind this insight. Figure 1 further illustrates this philosophy: by reducing the suicidal risk of the population at large (shifting the distribution of the suicidal risk of the whole population to the left), fewer people will have a very high risk of suicide (reduction in the area under the 'danger zone'). Hence, a partnership among mental health professionals and different sectors of the community should target the larger populations before 'symptoms' appear and the risk of suicide becomes imminent.
Some Local Research Findings
The aim of the HKJC Centre for Suicide Research and Prevention is to work with stakeholders in the community to search for evidence-based, innovative, and effective ways to prevent the tragic deaths. Research conducted by the HKJC Centre for Suicide Research and Prevention during the past 3 years has shown that the risk factors for suicide and suicidal behaviour are multiple in nature.
The risk factors are mainly psychiatric problems, unemployment, unmanageable debts, poor social problem- solving skills, and being separated, divorced, widowed, or never-married. Depression is also an important risk factor for suicidal behaviour.3 On the other hand, good coping strategies, strong family and social support systems, and social connectedness, as well as responsibility to the family as a reason for living, make people become more resilient to adverse life situations.
On the basis of these findings, a reduction in the suicide rate should be possible if the mental health of the general population and services for high-risk groups can be improved. Furthermore, suicide prevention efforts need to address the multiple causes of suicide and suicidal behaviour by using all possible avenues. Such efforts may include en- hancing mental health education, empowering families to function better, improving community network support, and, more specifically, restricting access to the means of com- mitting suicide.
An example of a successful community-based suicide prevention effort can be found in Cheung Chau Island, which is a popular getaway destination in Hong Kong. After a local visitor committed suicide by burning charcoal in a holiday flat in 1998, the island became notorious as a popu- lar place to commit suicide. To tackle the problem, the local representatives of the island initiated a joint effort to prevent further suicides, which involved a partnership among community members, the police, and mental health care professionals. In the 2 years after the programme's implementation, the number of suicides decreased sub- stantially. The experience illustrated the effectiveness of timely in-person crisis intervention and community-based gate keeping in preventing suicide, and strengthened the belief that suicide is preventable. Prevention needs the in- volvement of the whole community and volunteers within the community. Implementing a neighbourhood watch scheme and strengthening the community network seem to be promising measures to prevent suicide at the community level.
The Way Forward
In the past few years, Hong Kong has witnessed enormous progress in suicide prevention work initiated by the government, Hospital Authority, non-governmental organisations, academic institutions, and individuals in the community. It is time for these groups to join efforts and work towards an integrated, holistic strategy of suicide prevention. This approach has been taken by many differ- ent countries: the USA, England, Scotland, Australia, New Zealand, Finland, and Norway are among the countries that have developed comprehensive national suicide prevention strategies that incorporate a public health approach. National strategies for suicide prevention in these countries share a number of common elements, which include the use of educational settings as sites of intervention; attempts to change the portrayal of suicidal behaviour and mental illness in the media; efforts to increase and improve the detection and treatment of depression and other mental illness; an empha- sis on reducing the stigma associated with help-seeking behaviours; strategies designed to improve access to services; promotion of effective preventive efforts with rigorous evaluation; and efforts to reduce access to means of suicide.8 Learning from other countries, Hong Kong should place great value on implementing a similar public health approach.
The need for an effective suicide prevention programme in Hong Kong is clear. However, one of the most challeng- ing concerns to offering a suicide prevention programme is the lack of objective evidence on the effectiveness of the programme.13 Policymakers and stakeholders often do not have adequate information on what makes an effective pre- vention programme. It cannot be stressed enough that evalu- ation is highly important and essential in directing scarce resources to their appropriate use, as well as in constant improvement of services. Therefore, there is an urgent need to develop local skills for rigorous evaluation and to make evaluation a necessary, rather than auxiliary, component of local prevention efforts.
A measure of the effectiveness of suicide prevention efforts is the reduction in the level of suicidal behaviour in the community. Accurate surveillance and monitoring of suicide and suicidal behaviour is crucial. As in any surveil- lance and monitoring system, constant effort is needed to ensure the reliability and validity of the data.
The WHO acknowledges that the principle of connec- tedness is important in designing suicide prevention programmes.2 Restoring the connectedness between people and their communities, workplaces, and families is not only the key to suicide prevention; it should also be the guiding principle for stakeholders to work together. The slogan of the World Suicide Prevention Day on 10 September 2005 is "Prevention of suicide is everybody's business". 9 I sincerely appeal to everyone for continued support of local suicide prevention efforts, especially because all of us have an important stake in this endeavour.
Acknowledgements
The author is grateful to the support from the Chief Execu- tive Community Project and the Hong Kong Jockey Club, to the staff of the Hong Kong Jockey Club Centre for Sui- cide Research and Prevention, and to KY Liu for comments on an earlier draft of this paper.
References
- World Health Organization (WHO). World report on violence and health.
- Geneva: WHO; 2002.
- WHO. Suicide huge but preventable public health problem, say WHO. Geneva: WHO; 2004. http://www.who.int/mediacentre/news/releases/2004/pr61/en
- Hong Kong Jockey Club Centre for Suicide Research and Prevention. Research findings into suicide and its prevention: final report, 2005 July. Hong Kong: Hong Kong Jockey Club Centre for Suicide Research and Prevention; 2005.
- Mercy JA, Rosenberg ML. Building a foundation for suicide prevention: The contributions of Jack C. Smith. Am J Preventive Med 2000;19 (Suppl):26-30.
- Hawton K. A national target for reducing suicide. BMJ 1998;317: 156-157.
- Lewis G, Hawton K, Jones P. Strategies for preventing suicide. Br J Psychiatry 1997;171:351-354.
- Maris R. Pathways to suicide. Baltimore: Johns Hopkins University Press; 1981.
- US Department of Health and Human Services. National strategy for suicide prevention: goals and objectives for action. Rockville: US De- partment of Health and Human Services; 2001. http://www.who.int/mediacentre/news/releases/2004/pr61/en/
- International Association of Suicide Prevention. World suicide prevention day: prevention of suicide is everybody's business. International Association of Suicide Prevention; 2005. http://www.med.uio.no/iasp/wspd/WSPD2005brochureEnglish.pdf
- Gordon R. An operational classification of disease prevention. In: Steinberg JA, Silverman MM, editors. Prevention of mental disorder. Rockville: US Department of Health and Human Services; 1987:20-26. Dorwart RA, Ostacher MJ. A community psychiatry approach to pre- venting suicide. In: Jacobs DG, editor. The Harvard Medical School guide to suicide assessment and intervention. San Francisco: US Jossey- Bass/Pfeiffer; 1998:52-71.
- Rose G. The strategy of preventive medicine. Oxford: Oxford University Press; 1992:24.
- Gunnell D, Frankel S. Prevention of suicide: aspirations and evidence. BMJ 1994;308:1227-1233.
