
J.H.K.C. Psych. (1994) 4, 12-19
ORIGINAL PAPER
SUMMARY
A preliminary report of a study of verbal working memory in 161 schizophrenic patients is presented. We aim to resolve conflicting findings in previous studies by employing a larger sample size. An impairment in verbal working memory is found in our sample of schizophrenic patients. This impairment is not related to positive symptoms, negative symptoms, or formal thought disorder. It is present in patient who are free of anti-psychotic and anti-cholinergic medications. The neurobiological and functional implications of this finding are discussed.
INTRODUCTION
It is become increasingly recognized that schizophrenia is associated with a wide range of cognitive abnormalities (e.g. Strauss, M.E., 1993; Saykin et al, 1994; Goldberg et al, 1993; Gruzelier et al, 1988). The nature and extent of cognitive impairment in schizophrenia has been a subject of intense study in recent decades. One area of debate is whether psychological impairment in schizophrenia has a specific profile {i.e. consistently affecting different functions to different extents), or whether the impaim1ent is nonspecific {e.g. Saykin et al, 1991; Clare et al, 1993;). While impairment in a large number of psychological functions e.g. semantic memory, verbal memory, executive functions has been reported, one of the few areas where investigators often found unimpaired in schizophrenia is working memory, especially, verbal working memory {see below). Unimpaired verbal working memory {as is claimed by most studies) in the background of widespread deficits in other psychological function may therefore provide important insight in the understanding of the nature of cognitive impairment in schizophrenia.
WORKING MEMORY
Working memory is a cognitive system involved in temporarily holding and manipulating information. A widely accepted theoretical model on working memory has been proposed by Baddeley and Hitch {see Baddeley, 1990). Working memory has been considered as a limited-capacity system comp1ising a "central executive" that supervises and coordinates subsidiary "slave" systems. "Slave systems" are responsible for temporary storage of information in particular modalities. Two of the most studied "slave systems" are the "phonological loop" and the "visual-spatial sketch pad" {Baddeley, 1986, 1990; Hitch, 1984). While the fo1mer is concerned withverbal information, the later is concerned with visual and spatial information. Evidence of the dissociation of "phonological loop" and "visual-spatial sketch pad" comes from studies on brain injured patients (Vallar & Baddeley, 1984; Baddeley, 1990).
Verbal information can be held within a phonological store for a limited duration. They are maintained within the store via a process of subvocal rehearsal or articulation. Experimental characterization for the "phonological loop" comes from studies by Baddeley (1986), Baddeley, Thomson & Buchmanan ( 1975). Digit span has been widely used as a measure of verbal working memory and thus reflects the functioning of the "phonological loop" {Baddeley, 1986; 1990). While verbal working memory could also be assessed by testing other verbal items such as words or letter, words are more susceptible to interference from semantic effects, and letters have no equivalent in Cantonese. Digit span has the advantage of being neutral in meaning, and that norms for digit span are available in Cantonese as well as in English.
Digit span is divided into fo1ward digit span and backward digit span. The former is the maximum number of digits a subject could repeat in the 01iginal order immediately after presentation. Backward digit span requires a subjects to recall the numbers in the reversed order. Backward digit span also involves a visualization of the number digits and conversion into spatial coordinates (Rudel and Denckla, 1971).
VERBAL WORKING MEMORY IN SCHIZOPHRENIA
Several studies on schizophrenic patients examining cognitive performance indicate that functioning of the phonological loop is probably preserved. Park and Holzman (1992) studied the working memory of 12 schizophrenic, 12 bipolar and 12 normal subjects. With a small sample size, significant difference was found among the three groups on fo1ward and backward digit span. In contrast they demonstrated an impairment of spatial working memory in patients. McKenna et al (1990) found that 51 out of 60 schizophrenic subjects "passed" the fo1ward digit span subtest of the Middlesex Elderly Assessment of Mental State, sc01ing "five" and all the other patients scored "four". A more detailed case study of five memory impaired patients revealed that they showed a typical minor detrimental effects of phonemic simila1ity (Tamlyn et al, 1992), suggesting that the phonological loop was functioning norn1ally. Duffy & Carroll (1994) also repo1ted that in 40 schizophrenic patients forward digit span fell within a normal range of five to nine digits. This is observed in the background of markedly impaired long-term memory. On the other hand, Gruzelier et al (1988) reported a significant difference in fo1ward digit span between 36 schizophrenics and 29 normal controls.
Studies employing both f01ward and backward digit spans suggested a possible poorer perforn1ance over backward digit span test. Again, results from previous studies are conflicting. Braga & Neufeld (1981) combining the result of fo1ward and backward digit spans, reported no significant difference between 20 paranoid, 20 non-paranoid schizophrenics and 40 normal subjects. However, Goldberg et al. (1993) examined 24 rnonozygotic twin pairs discordant for schizophrenic or delusional disorder and seven norn1al monozygotic twins pairs and found no significant difference over f01ward digit span but signif-icant difference was identified in the backward digit span. A further interesting observation comes from Franzen & Ingvar's study (1975) which found a significant lower reg-ional cerebral blood flow over frontal regions in schizo-phrenic patients when testing backward digit span. As testing on backward digit span involves visual transformat-ion, it is possible that poor visual transform-ation may be related to impaired perforn1ance in schizophrenic patients.
Unfortunately the interpretations of digit span data from most previous studies are often compromised by small numbers of subjects. Another potential source of difficulty might lie in the sensitivity of digit span as a measure of verbal working memory. Impairment has to be at least one digit in magnitude in order to be detected. One digit is a significant amount in the context of a normal digit span of seven (i.e. impairn1ents are detected only if they are greater than 14%).
Normal digit span is language-dependent (Ellis and Hennelley, 1980). In Cantonese speaking subjects, a potential advantage offered to the investigator is the larger number of digits achieved in the normal span (forward span: over nine digits). Hoosain (1979 & 1984a) consistently found a larger forward and backward digit span when the bilingual subjects performed digit span tests in Cantonese than that in English. This is presumably due to the reduction in time taken to a1ticulate digits in Cantonese. Hoosain (1984b) found a overall shorter duration of pronouncing digits in Cantonese than in English by native speakers. It is possible that this larger normal digit span may render the Cantonese test more sensitive than the equivalent test in English.
In this study we investigate digit span for Cantonese speaking schizophrenic patients. We employed a larger sample of patient in order to ensure sufficient statistical power of the study as well as to enable study of relationship between verbal working memory and some other clinical variables.
METHOD
SUBJECTS
161 patients aged between 16 and 65 were rec11.1ited from inpatient psychiatric units. The diagnosis of schizophrenia was made according to DSM-III-R c1ite1ia (Ame1ican Psychiat1ic Association, 1987) based on information obtained from clinical interview and medical records. Patients were excluded if they have organic brain disease (such as epilepsy and cerebrovascular disease), mental retardation, head injury, alcohol or d11.1g abuse, or if they had received electroconvulsive therapy within the last 6 months. All patients gave informed consent to the assessment. Fo1ward and backward digit span data was also obtained for 95 normal volunteers.
PROCEDURE
Digit spans were assessed following the standard procedure desc1ibed in the Wechlser Adult Intelligence Scale. The subjects were given inst11.1ctions to repeat the sequence of digit immediately after they had been read out to them. The monosyllabic digits in Cantonese were read out in the rate of one per second. Sequences of digits were read out sta1ting with the sh01ter sequences. When the subject successfully completed two sequences of a ce1iain length (e.g. two 4-digit sequences), it was followed by sequences one digit longer (i.e. 5-digit seque-nces). This carried on until the subject failed on both sequences of the same length at which point the test terminated.
Assessment of digit span was carried out as pa1t of a broader study investigating the neuropsychological and neurological impairment of schizophrenic patients. Clinical information was obtained by interview with the patient: psychotic symptoms were assessed using Comprehensive Assessment of Symptoms and History (CASH, Andreasen, 1987), negative symptoms using the High Royds Evaluation of Negativity (HEN, Mo1timer et al, 1989). Global symptom profile was assessed using the Brief Psychiatric Rating Scale (BPRS, Overall and Gorham, 1962). Antipsychotic medication dosages were converted into daily chlorpromazine equivalent according to Davies (1974). Chronicity of ilh1ess is expressed as the number of years since first hospitalization. Assessment of digit span was carried out by researchers blind to clinical information.
RESULTS
DIGIT SPAN COMPARISON WITH CONTROLS
Forward and backward digit spans in 161 schizophrenic patients compared with those of 95 control subjects are shown in figure one. There is a clear difference between patient and control in both forward and backward spans (See Table 1).
RELATIONSHIP WITH SYMPTOMS AND OTHER CLINICAL VARIABLES
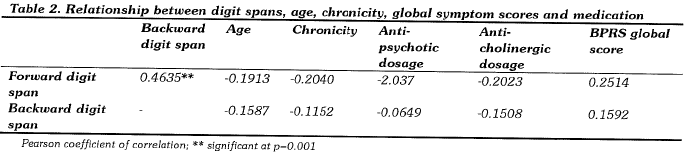
For schizophrenic patients analysis of correlation was carried out between digit spans and other clinical variables. There was a significant correlation between performances in the forward and the backward digit spans. There was no correlation between digit spans and age, BPRS global scores, anti-psychotic medication dosage, anti-cholinergic medication dosage, or chronicity of illness (Pearson correlation coefficients, significant level at 0.001: a more stringent significance level is chosen to minimize the effects of spurious correlations).
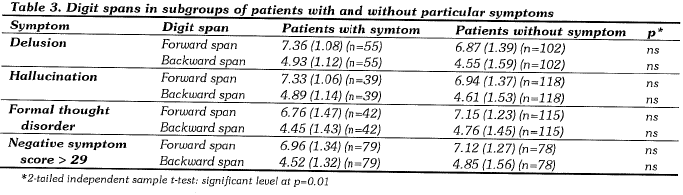
SYMPTOMS OF DELUSION, HALLUCINATION FORMAL THOUGHT DISORDER AND NEGATIVE SYMPTOMS
Further analysis was carried out investigating the relationship between digit span and individual symptoms. For each symptom of interest (delusions, hallucinations and formal thought disorder), patients were divided into two groups according to whether they exhibit the symptoms or not. Digit spans for the two groups (with and without the symptom in question) are then compared (two-tailed independent t-tests, significance level 0.01). There is no significant difference in forward and backward digit spans between the groups for each of the symptom considered (See Table 3).
PATIENTS WITH HIGHER LEVEL OF EDUCATION
To investigate whether the relatively low level of education in patients might confound our findings, further analysis was carried out on a subgroup of 39 patients who has more than 11 years of education (post-secondary). The difference in digit spans still remains between this group of patients and controls (See Table 4).
MEDICATION- FREE PATIENTS
From the schizophrenic patient sample, 12 patients who has been medication free was selected for further compa1ison. In addition the digit spans of 59 patients who received no anti-cholinergic medication were compared with controls. Both groups of patient (no anti-psychotic and no anticholinergic) still showed a significant reduction in their verbal memory spans compared with controls (Table 4 ).
FIRST-EPISODE MEDICATION-FREE PATIENTS
A subgroup of six first-episode medication-free patients are identified from the sample. Although the number of first-episode medication-free subjects is small in our sample, it can be seem that their mean forward and backward digit spans are similar to those of the rest of the patient sample and different from the controls (Table 4).


DISCUSSION
These preliminary results suggest that verbal working memory spans as measured by digit spans are impaired in schizophrenic patients. The finding is consistent with those of Gruzelier et al (1988) but differs from other published reporis based on studies with a smaller sample size (which generally repo1ied failures to detect impairments). The use of a more sensitive Cantonese-based digit span assessment and the use of a larger sample size might underlie our ability to detect a modest impairment in digit spans in schizophrenic patients.
Our larger sample size also enables some fu1iher analysis on the relationship between digit span impairments and other clinical va1iables. There is no significant association between digit span performance and positive symptoms, negative symptoms or formal thought disorder. This suggest that impairment in digit span is not directly related to symptoms and could not be entirely att1ibuted to distraction by symptoms.
Anti-psychotic and anti-cholinergic medication potentially could affect cognitive performance (e.g. Sweeney et al, 1991). However we found that there is no correlation between dosages in these medication and digit span performance. Furthermore when patients free of these medication are studied, the same pattern of verbal working memory impairment is still apparent. These observation suggest that working memory impairment is intrinsically related to the schizophrenic illness rather than a result of medication treatment.
Impairment in verbal working memory performance in schizophrenia is in agreement with current neurobiological understanding of the disorder. Working memory is mediated by a neural circuit involving the prefrontal cortex, thalamus, parietal cortex and the basal ganglia (GoldmanRakic et al, 1991). Neuropsychological studies also confirm the involvement of prefrontal cortex in digit span performance (Shimamura et al, 1991). In schizophrenia there is strong evidence from functional imaging studies implicating abnormal prefrontal cortical function (Berman et al, 1988; Weinberger et al, 1991). This is consistent with findings of other "executive" type of neuropsych-logical impai1ment. In this context, verbal working memory impairment may be considered as a further neuropsychological marker (and one that can be easily measured clinically) for the disorder.
Implications of verbal working memory impairment in schizophrenia is not restricted to neurobiological and neuropsychological issues. Working memory is an important aspect of ordinary everyday psychological functioning. As working memory reflects the amount of information that could be processed at the same time, it has important bea1ing on the ability to analyze and interpret complex environmental inputs, as well as the planning of structured, ordered sequence of action. In addition, there is evidence t11at prefrontal cortex mediated working memory and related functions may be involved in complex emotional and motivational responses (Damasio et al, 1991). Clinically it is not difficult to identity patients with disability in one or more of these areas. These disabilities may contribute significantly to the social and occupational handicap associated with schizophrenia. Better understanding of these deficits would be essential for a rational approach to rehabilitation.
Fu1iher work will be required to characterize working memory impai1ment in schizophrenia. For example the relationship between verbal working memory impairment and non-verbal working memory impairment deserves investigation. Although age (except in the very young and the elderly) is generally not regarded as a variable confounding digit spans performance {Craik, 1977), it may complicates the analysis of the effects of chronicity of illness. We are current enlarging the sample size so that multiva1iate technique could be applied to address some of these issues.
A preliminary report is presented of a study of verbal working memory in schizophrenic patients. Compared with previous studies a larger sample size and a more sensitive method were used exploiting the larger normal digit span in the Cantonese language. An impairn1ent in verbal working memory is found in schizophrenic patients. This impairment is not related to positive symptoms, negative symptoms, or formal thought disorder. It is present in patient who are free of anti-psychotic and anti-cholinergic medications. Further characte1ization of this impairment will be possible with an extension of the sample size.
ACKNOWLEDGMENT
This research has been carried out with the support of a grant from the University of Hong Kong!
REFERENCE
Andreasen, N.C. (1987) The Comprehensive Assessment of Symptoms and History. University of Iowa College of Medicine: Iowa City.
Baddeley, AD. (1990) Human Memory: theory and practice.
Sussex: Lawrence Erlbaum Associates.
Baddeley, AD. (1986). Working Memory. New York: Oxford University Press.
Baddeley, A.O., Thomson, N. & Buchmanan,M. (1975). Word length and the structure of short-term memory. Journal of Verbal Learning and Verbal Behaviour, 14, 575-589.
Berman 1-<F, Illowsky BP, Weinberger DR (1988): Psychiological dysfunction of dorsolateral prefrontal cortex in schizophrenia: JV further evidence for regional and behavioral specificity. Arch Gen Psychiatry 45:616-622.
Braga, M.I. & Neufeld, R.W.J. (1981). Multivariate cognitive performance lecels and response styles among paranoid and nonparanoid schizophrenics. Journal of Abnormal Psychology, 90 (6), 495-509.
Clare, L., McKenna, P.J., Mo1iimer, A.M., and Baddeley, A.O. (1993) Memory in schizophrenia: what is impaired and what is preserved? Neuropsychologia 31: 1225-1241.
Craik, F.I.M. (1977) Age differences in human memory. In Handbook of the psychology of aging (eds. Birren, J.E. and Schaie, KW.) van Nostrand Reinhold, New York.
Damasio AR, Tranel D, Damasio HC.(1991) Somatic markers and the guidance of behavious: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL. eds. Frontal lobe function and dysfunction. Oxford: Oxford University Press; p. 217-229.
Davies, J.M. (1974) Dose equivalence of the anti-psychotic drugs.
Journal of Psychiatric Research. 11, 65-69. ·
Duffy, L. & O'Canoll, R. (1994) Memory impairment in schizophrenia : a comparison with thot observed in the alcoholic
Korsakoff syndrome, Psyhological Medicine, 24(1): 155-166.
Ellis, N.C. and Hennelley, R.A. (1980) A bilingual word-length effect: implications for intelligence testing and the relative ease of mental calculation in Welsh and English. British Journal of Psychology, 71, 43-52.
Franzen, G. & lngvar, D.H. (1975). Absence of activation in frontal structures during psychological testing of chronic schizophrenics, Journal of Neurology, Neurosurgery, and Psychiatry, 38, 1027-1032.
Goldberg, T.E., Toney, E.F. Gold, J.M., Tagland, J.D., Bigelow, L.B. & Weinberger, D.R. (1993). Learning and memory in monozygotic twins discordant for schizophrenia, Psychological Medicine, 23, 71-85.
Goldman-Rakic PS, Friedman HR. The circuitry of working memory revealed by anatomy and metabolic imaging. In: Levin HS, Eisenberg HM, Benton AL. eds. Frontal lobe function and dysfunction. Oxford: Oxford University Press; 1991:72- 91.
Gruzelier, ,J., Seymour, K, Wilson, L., Jolley, A., & Hirsch, S. (1988) Impairments on neuropsychologic tests of temporohippocampal and frontohippocampal functions and word fluency in remitting schizophrenia and affective disorders, Archives of General Psychiatry, 45, 623-629.
Hitch, G.J. (1984). Working memory. Psychological Medicine, 14, 265-271.
Hoff , AL., Riordan, H., O'Konnell, D.W., Morris, L. & Delist, LE. (1992), Neuropsychological functioning of first-episode schizophreniform patients. American Journal of Psychiatry, 149(7), 898-903.
Hoosain, R. (1979). Forward and backward digit span in the languages of the bilingual. Journal of Genetic Psychology, 135, 263-268.
Hoosain, R. (1984a). Lateralization of bilingual digit span functions, Perceptual and Motor Skills, 58, 21-22.
Hoosain, R. (1984b). Psychological studies of the Chinese language. Hong Kong: Tai Do Publishing.
McKenna, P.J. Tamlyn, D., Lund, C.E., Mortimer, A.M. Hammond, S. & Baddeley, A.O. (1990),. Amnesic syndrome in schizophrenia. Psychological Medicine, 20, 967-972.
Mortimer, AM., Lund, C.E., McKenna, P.J. & Mannuzza S (1989) Rating of negative symptoms using the HEN sale: British Journal of Psychiatry, 155, suppl. 7, 89-92.
Overall, J.E. and Gorham, D.R. (1962) The Brief Psychiatric Rating Scale. Psychological Reports, 10, 799-812.
Park, S. & Holzman, P.S. (1992) Schizophrenics Show Spatial Working Memory Deficits. Archives of General Psychiatry, 49, 975-982.
Rudel, R.G. & Denckla, M.B. (1974). Telationof forward and backward digit repetition to neurological impairment in children with learning disabilities. Neuropsychologia, 12, 109-118.
Saykin, A.J., Gur, R C., Gur, RE., Mozley, P.O., Mozley, L.H., Resnick, S.M., !Zester, D.B. and Stafiniak, P. (1991) Neuropsychological function in schizophrenia: selective impairment in memory and learning. Archieves of General Psychiatry 48, 618-624.
Saykin, A.J, Shtasel, D.L., Gur, R.E.Kester, D.B., Mozley, L.H., Stafiniak, P and Gur, R C. (1994) Neuropsychological deficits in neuroleptic naive patients with first-episode schizophrenia. Archives of General Psychiatry, 51, 124-131.
Shimamura AP, Janowsky JS, Squire L (1991): What is the role of frontal lobe damage in memory disorders?. In Levin HS, Eisenberg HM, Benton AL (eds)Frontal lobe function and dysfunction, Oxford: Oxford University Press, pp. 173-198.
Strauss, M.E. (1993) Relations of symptoms to cognitive deficits in schizophrenia. Schizopluenia bulletin 19(2): 215-231.
Sweeney, J.A, Keilp, J.G., Haas, G.L. Hill, J. and Weiden, P.J. (1991) Relationships between medication treatments and neu- ropsychological test performance in schizophrenia. Psychiatry Research, 37: 297-308.
Tamlyn, D., McKenna, P.J., Mortimer, AM., Lund, C.E. , Hammond, S. & Baddeley, AD. (1992). Memory impairment in schizophrenia: its extent, affiliations and neuropsychological character. Psychological Medicine, 22, 101-115.
Weinberger DR, Berman KF & Daniel DG (1991): Prefrontal cortex dysfunction in schizophrenia. In Levin HS, Eisenberg HM, Benton AL (eds) rontal lobe function and dysfunction, Oxford: Oxford University Press, pp. 275-287.
*Eric Y.H. Chen MBChB, MA(Oxon), MRCPsych Lecturer, Department of Psychiatry, University of Hong Kong.
Charlotte K.Y. Chan BA Research Assistant, Department of Psychiatry, University of Hong Kong.
Ronald Y.L. Chen MBBS Lecturer, Department of Psychiatry, University of Hong Kong.
Desmond G.H. Nguyen MBBS Medical Officer, Kwai Chung Hospital
Linda C.W. Lam MBChB, MRCPsych Lecturer, Department of Psychiatry, Chinese University of Hong Kong.
*Correspondence: Dr. Eric Y.H. Chen, c/o : Department of Psychiatry, Queen Mary Hospital, Pokfulam, Hong Kong.
