
Hong Kong Journal of Psychiatry (1997) 7 (1),25-27
SPECIAL TOPIC: Benzodiazepines - Uses & Abuses
Summary
Benzodiazepines , with it’s propensity of abuse proven and the prescription practice of clinicians often put to blame by the public, official guidelines are prepared and whose controversy has been argued extensively. The importance of surveys of BZD abuse in the medical populations and BZD prescription practice have been stressed. Brief mention is made on BZD abuse in the local scene of polydrug abuse.
Keywords: abuse, tolerance, dependence, withdrawal, multiple drug abusers
INTRODUCTION
Benzodiazepines (BZD) has been introduced into clinical practice since 1960. The popularity of these medication with clinicians and patients appears to be its actions ·against the ubiquitous symptoms of anxiety, relative safety, and its ability to stimulate and reinforce its own taking in users, and the propensity to produce pharmacological tolerance and dependence. The evidence of harm to users has been cleared, which not only includes that of dependence, but its adverse effects of cognition, psychomotor performance and disinhibition with aggressiveness and suicide. Epidemiological studies in western countries did point to the evidence of non medical use or abuse in the general population. Prescription practice among clinicians are surveyed. Good practice of prescription of BZD and methods of withdrawal are promoted. Yet, all these have not happened in Hong Kong till recently. A doctor in court, when challenged of his prescription practice a few years ago, had made reference to his textbook of the 60s that BZD is described to be safe and not having any dependence potential. This did sound a warning to our profession.
However, it's only when the sensationalistic media, which has shown great interest in the doctor-peddlers in their profit making sale of BZD, asserts the existence of a major health problem generated by the medical malpractice and indicating our profession is urgently required to do something, i.e. by issuing a set of guidelines of the use of the drug. And this has been done but unavoidably, in so doing, an impression is obviously been made to the public that our profession has not been practicing properly all the time and thus creating opportunity of drug peddling. It could have been far better if we could have performed a survey on our prescription practice, thus proving that it is only the ten or twenty black sheep of the profession who are deviating from the normal clinical practice. After that, a guideline of facilitative nature can be promoted to the profession, and not a restrictive one. This is because the ordinary clinician would react to the present set of official guidelines by a simple withdrawal from its prescription but pay little attention to the risk of abrupt withdrawal in their clients. They would blame the body preparing the guidelines, who has the sole intention of stopping the doctor-peddlers. This makes such restrictive guidelines very unlikely to succeed.
BZD ABUSE - THE CURRENT SCENE
Now, let us turm to the very topic of 'BZD abuse - the current scene'. What is abuse? Definitions of abuse varies. Use and abuse form a rather uncertain continuum. The following are 2 definitions which I would recommend:
Applying these 2 sets of definition, it is easy to decide on abuse, i.e. it is non-medical and doing harm or potential harm to self or to the society. Yet, the question of the appropriateness of the therapeutic indications may not be so clear and is of great concern in our daily practice. A key to it would be a determination of the risk-benefit ratio for BZD user. However, it might be controversial if it is applied to patients using therapeutic doses of BZD over long periods of time, who do not become intoxicated, and do not experience any impairment of social or occupational functioning, but not to forget, such individual may be exposed to the risk of physical and psychological dependence.
Lets look at the drug itself. BZD have been found to have some abuse potential, but less than that of barbiturates which they have replaced. Studies of abuse potential in humans have considered diazepam and triazolam to have similar abuse potentials, based on rating of euphoria and drug liking by subjects with histories of sedative abuse. Generally speaking, slowly absorbed BZD, including chlordiazepoxide, chlorazepate, halazepam, oxazepam, and prazepam, seem to have a lower abuse potential than other BZD including alprazolam, diazepam, lorazepam, and triazolam., which have a more rapid onset of action. Epidemiological studies also show that BZD have a lower abuse potential in the general population, but that their abuse potential is increased for abusers of alcohol and other drugs like heroin and cocaine.
What about the abuse patterns? There are 2 groups: those who use only BZD and those who use BZD in the context of multiple drugs. The former are older in age and took significantly lower doses of BZD than multiple drug users. The first group uses BZD for therapeutic indications for a length of time beyond recommended medical practice and the other uses BZD in high doses among other drugs in an abusive manner. This is consistent with my observation and findings in the 2 Substance abuse clinic services in the past 2 years (Annual report KHSAC, 1994; Annual report TMSAC, 1995). The first group tends to be more of the female sex. The latter group has no sex preference and abuses BZD sporadically, without dependence physically, and using it either in combination with heroin to boost the euphoria or sporadically to sedate or for better sleep, especially during abstinence.
LOCAL DATA
What about the local scene? Local epidemiological studies are sadly lacking, in regard to the group of BZD abusers who have been using the drug for long period of time beyond recommended practice, and not infrequently obtaining from multiple sources. One cannot obtain any meaningful statistics from the public health related departments or authority. Morbidity statistics provides data only on 'drug dependence" and without breakdown into the kinds of drug concerned. There has never been any survey of BZD prescription practice from general practitioners, psychiatrists or neurologist or internist.
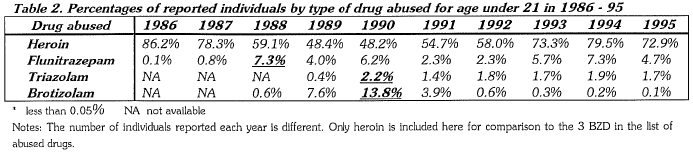
Concerning the polydrug-BZD abusers, some meaningful data can be provided. The Central Registry of Drug Abuse, (CRDA) 37th Report shows that in 1995, 89.2% of reported individuals of all ages abused heroin, followed with 8% for cough mixture, 7.8% for cannabis, 2.2% for Triazolam and 1.6% for Flunitrazepam (See Table 1). Data for reported individuals under 21 are similar, except that it is higher for cannabis (20%) and there is a reversal of order for Flunitrazepam (4.7%) over Triazolam (1.7%). From the CRDA data, Flunitrazepam and Triazolam are the most abused BZD, and Flunitrazepam is of favour for the under 21 age group (See Table 2). The abuse of Brotizolam, a kind of BDZ normally not of clinicians' choice, has been decreasing in popularity. Its popularity gained some years ago was because of its categorization as scheduled drugs instead of dangerous drugs like other BDZ, thus making it easier to be obtained in pharmacy. Of course, this had been rectified soon afterwards.
Another source of information is from the drug seizures of Police & Customs. The 4 largest seized BZD are Flunitrazepam, Triazolam, Midazolam and Lorazepam. The Government chemist has also given some stunning data of fake Flunitrazepam, consisting of 2 mg of Triazolam instead of the supposed 2 mg of Flunitrazeapm per tablet, i.e. one is taking 2 mg of triazolam while intending to have 2 mg of Flunitrazepam, and which means 8 times of normal dose of 0.25 mg Triazolam, or 16 times a lower normal dose of 0.125 mg Triazolam (a lower dose of Triazolam as hypnotic is advocated). Taking multiple tablets of the fake Flunitrazepam is obviously hazardous and been proven fatal in a case reported. Government chemist also has the impression that finding BZD in urine screening of drug abusers is uncommon while admitting that detection of BZD is difficult in view of its minute quantity in urine sample. As it is only the metabolites which are or can be screened, it is impossible to identify the kind of BZD abused. One point of interest concerning Midazolam is that it is commonly mixed with heroin according to the heroin seized by the Police and Customs.

CONCLUDING REMARKS
It may not be necessary to make special request of anyone of you to follow any of the guidelines of BZD prescription, as I am sure you are already practicing with the principles adopted, but there is a cogent need to call for conducting surveys of BZD abuse/dependence in the general or medical populations, or studies of the BZD prescription practice of doctors. Coop eration of doctors in doing such survey or study should be for the sake of the medical profession. I hope that its result can rectify the allegations of the sensationalistic media that our prescription practice has been the cause of abuse and causing harm to public health. If, on the contrary, the finding indicates that our medical population has being prescribed with BZD not for the definable medical condition but for the malaise and anomie that comes from an unsatisfactory social situation or unresolved personal problems, we must admit to our part in 'drugging the society', a practice of grave implication.
REFERENCES
The Royal College of Psychiatrists (1987) The Drug Scenes - A report on Drugs & Drug dependence by the Royal College of Psychiatrists.
Leung, S. P. (1994) Annual Report of Kowloon Hospital Substance Abuse Clinic, 1994.
Lam, M & Leung, S.P. (1995) Annual Report of Tuen Mun Substance Abuse Clinic, 1995.
Narcotic Division, Government Secretariat, Hong Kong. Central Registry of Drug Abuse, 37th Report, 1986 -1995.
Leung Shung Pun MBBS, MRCPsych, FHKAM (Psychiatry) Chief of Service, Castle Peak Hospital, Tuen Mun, N. T. Hong Kong.
This paper is presented in the scientific symposium on "Benzodiazepines Controversies: from use to abuse" organized by the Hong Kong College of Psychiatrists on 12 June 1996.
