
Hong Kong J Psychiatry 2003;13:2-7
ORIGINAL ARTICLE
CWY Chan, LCW Lam, TCM Wong, HFK Chiu
Abstract
Objective: To examine the performance of Nelson’s Modified Card Sorting Test in community dwelling elderly Chinese people.
Patients and Methods: Nelson’s Modified Card Sorting Test was administered to 95 healthy elderly Chinese people. Relationships between the Modified Card Sorting Test performance and demographic characteristics were evaluated.
Results: Most people (86.3%) were unable to complete 6 categories, and many of them made perseverative errors. Approximately 30% made more than 50% perseverative errors. Age, educational level, and gender significantly affected Modified Card Sorting Test performances, with education demonstrating the largest effect on performance.
Conclusion: These findings suggest that demographic factors appear to exert a significant impact on Modified Card Sorting Test performances in elderly people, so these should be taken into consideration during interpretation of clinical assessments. For the effective use of the Modified Card Sorting Test in clinical settings, further studies of specific clinical populations are required to develop normative data for elderly Chinese people.
Key words: Chinese, Demographic variables, Elderly
Dr CWY Chan, BSocSc, Department of Psychiatry, the Chinese University of Hong Kong, Hong Kong, China.
Dr LCW Lam, MRC Psych, FHKC Psych, FHKAM (Psychiatry), Department of Psychiatry, the Chinese University of Hong Kong, Hong Kong, China.
Dr TCM Wong, M Phil, Department of Psychiatry, Shatin Hospital, Shatin, Hong Kong, China,
Dr HFK Chiu, FRCPsych, FHKC Psych, FHKAM (Psychiatry), Jockey Club Centre for Positive Ageing, Hong Kong, China.
Address for correspondence: Dr Linda Lam, Department of Psychiatry, The Chinese University of Hong Kong, No 9 Chuen On Road, Tai Po Hospital, Tai Po, New Territories, Hong Kong, China.
Tel: (852) 2607 6040; Fax: (852) 2667 1255; E-mail: cwlam@cuhk.edu.hk
Submitted: 24 March 2003; Accepted: 15 October 2003
Introduction
The Wisconsin Card Sorting Test (WCST) is commonly used in neuropsychological assessment as a measure of executive function.1 Despite its popularity, several shortcomings of the test have been highlighted, and it may be particularly difficult for use with elderly people. Various authors have commented on its abstract stimuli, arbitrary nature, and lengthy adminis- trative time, which may reduce the examinee’s motivation to complete the test, and that many examinees become confused when performing the test.2,3 Therefore, it has been recom- mended that a modified or shortened form of the WCST might be better for use as a tool in neuropsychological assessment.2-4
Nelson developed a considerably shorter alternative version of the test, the Modified Card Sorting Test (MCST). The MCST differs from the WCST in several ways.3 Firstly, the 128 response cards have been reduced to 48, consisting of 2 identical packs of 24 response cards, with each card sharing only one attribute with any of the 4 stimulus cards. Lineweaver et al claimed that the change allows the examiner’s feedback to provide unambiguous information to the respondent, and the participant’s sorting strategy can be easily deduced.5 Secondly, the MCST allows the participants to begin with whatever category they choose and complete the other 2 categories in a self-selected order.5 Thirdly, instead of 10 in the original version, Nelson reduced the number of consecutive correct responses required for completing a category to 6. Fourthly, following 6 consecutive correct sorts, the participant is informed to change the rule and is told to find a new sorting principle. Since overall cognitive performance and attention capacity declines with age,6,7 a test with a shorter completion time, and clear and simple instructions that are easier to understand will be particularly beneficial for elderly people. The modifications in the MCST are likely to allow elderly people to perform better as they increase the flexibility and reduce the ambiguity of the test.
The MCST performance has been investigated in various neurological patient groups, for example, in the determina- tion of executive function in patients with Alzheimer’s disease,4 schizophrenia,8 epilepsy, and vascular dementia.9-11 In Nelson’s original description, the MCST was able to distinguish patients with frontal lobe lesions from patients with non-frontal lobe lesions by providing a cut-off score.3 Van den Broek et al also demonstrated the ability of the MCST to differentiate patients with focal lesions from a healthy control group with a good sensitivity (45.6%) and high specificity (98.5%).12 Despite the wide use of MCST, its psychometric properties are still unclear. Some authors commented that the modifications of the MCST altered properties of the original WCST, and may be measuring different psychological functions.13 Therefore, results from the 2 tests may not be interchangeable, although the MCST has been widely used to assess the function of the frontal lobe clinically and experimentally.14
Research shows increasing interest in the relationships between MCST performance and demographic data. In Nelson’s primary description, a significant negative age effect on the overall performance of the MCST was found.3 Several recent researchers also demonstrated that age has negative effect, while education has a positive effect on MCST performance.5,15,16 Van de Broek et al reported signi- ficant relationships between MCST scores and performance on the Wechsler Adult Intelligence Scale.12
In contrast to the large amount of research done on the WCST, information regarding MCST performance on healthy people is relatively scarce, especially in Asian populations. Among the studies done for MCST, none have included Asian participants. While an older adult population is considered most likely to be assessed by MCST for the detection of cognitive decline,4 few reports studied primarily the performance on MCST of healthy elderly people. Moreove r, most studies recruited highly educated participants with a mean educational level of more than 12 years, and MCST performance among the relatively low education group is not well known.5,15,16
This study aims to investigate the performance of MCST in healthy elderly Chinese people. The influence of demographic characteristics on the performance was evaluated and discussed.
Patients and Methods
Participants
The participants were 95 healthy elderly volunteers (76 women and 19 men) recruited from the community as part of a study of the Neurocognitive Correlates of Behavioral and Psychological Symptoms in Alzheimer’s disease conducted by the Department of Psychiatry, The Chinese University of Hong Kong. All participants were ethnically Chinese. All participants underwent clinical assessments of medical and neurological examinations to confirm their normal health status before recruitment. They were also screened for significant depressed mood by the Cornell Scale for Depression in Dementia and cognitive impair- ment with the Chinese version of the Mini-Mental State Examination.17,18 Exclusion criteria included history of psychiatric or neurological illness, previous significant head injury, and history of previous exposure to neurotoxins.
Methods
A standardised version of the MCST was used as part of a comprehensive neuropsychological assessment. The standardised MCST consisted of 4 unique stimulus cards, and 2 sets of 24 response cards. The 4 stimulus cards were the same as those used in the WCST. Each set of the 24 response cards comprised cards that shared only one attribute with each of 3 stimulus cards, but shared no attribute with the fourth card (e.g. the same colour as the first, same form as the second, same number as the third, but with no similarity to the fourth card).
The administration procedure and instructions given to the participants were as follows:16
“There are 4 key cards, I want you to match each of the cards in these decks [examiner indicating the response cards] to one of the 4 key cards [indicate each of the stimulus cards], according to certain rules. However, I cannot tell you what the rule is. You have to find out by trying different rules. I will tell you whether your response is correct or not. You have to take the top card from the deck every time, and put it below the key card that you think it matches. If you are told you are wrong, just leave the card where you placed it, and try the next card. Now, let’s begin.” As all the participants are ethnically Chinese and all of them speak Cantonese, the instructions used throughout the administration procedure were translated into Chinese and conducted in Cantonese.
The initial category chosen by the participants was scored as correct, and subsequent responses scored accordingly. After 6 consecutive correct responses to the initial sorting principle, the participant was told “I want you to change the rule now, please use a different rule to match the cards.” This instruction was used every time the rule was changed.
The new category chosen by the participant was then scored as correct, and the same procedure was repeated, i.e. following 6 consecutive correct responses, the third category had to be attained. After the completion of the third sorting principle, the 3 categories were repeated in their original order (for example, if the participant completed the 3 categories in the order of colour, form, and then number initially, the next correct sort should be colour, followed by form, and then number in sequence). If, following the completion of 3 categories, the participant asked whether it was allowed to repeat a rule that had been used before, or wondered that all possible rules had been tried out, he or she was advised “Find a rule which is different from the rule you used last time”. The test was completed after the participant finished 6 categories, or when all the 48 response cards had been exhausted.
Scoring
The participant’s responses were entered into a scoring sheet according to the attribute shared with the stimulus cards. Responses were recorded by circle for the representative sorting principle, where C represents colour, F represents form, N represents number, and U represents unique, i.e. no sorting principle matched. The order of sorting principles chosen by the participant was also recorded.
The following measures were obtained from the MCST: number of categories achieved (Cat); total number of errors (E); perseverative error score (PE); non-perseverative error score (NPE); failure to maintain the set score (FinMS); the number of unique errors (UE); and the percentage of perseverative error (%PE). An error was scored as persevera- tive if it followed the same principle as the immediately preceding response, but did not correspond to the current correct principle. The failure to maintain the set score is the number of times that the participant makes 3 consecutive correct responses but fails to attain 6 correct responses for the completion of a category. Unique errors (called random sorts by Nelson3) are those not sorted according to colour, form, or number principles.
Results
The age of the participants ranged from 57 to 89 years (mean age, 71.1 years, standard deviation [SD], 7.47 years). The mean educational level was 5.43 years (SD, 5.04 years).
Among the 95 participants, 13 (13.7%) completed 6 categories. One did not complete any category (Figure 1). More than half of the participants (51.6%) completed at least 3 categories.
The distribution of perseverative errors is positively skewed while the number of non-perseverative errors is roughly a normal distribution. The number of perseverative errors ranged from 0 to 35, with a mean of 9.36, while the number of non-perseverative errors ranged from 0 to 24, with a mean of 12.04. Analysis with Wilcoxon signed rank test showed that non-perseverative errors accounted for most of the errors (z = -3.783, p < 0.0005). Among the 95 participants, 5 (5.3%) made no perseverative errors, while 1 made 100% perseverative errors.
For the 13 participants who completed 6 categories, 5 (38.5%) made no perseverative errors and 8 produced between 1 and 6 perseverative errors. Although these participants made only a small number of perseverative errors, due to the small number of total errors they nevertheless achieved a high percentage of perseverative errors from 20% to 100%. In these cases, the high %PE may not accurately reflect the degree of perseveration error. Therefore, it was considered inappropriate to analyse the percentage of perseverative errors for those who obtained few errors overall. As it is invalid to measure %PE when performance is maximal,3 the 13 participants who completed 6 categories were excluded in the analysis of %PE. Of the 82 participants who completed fewer than 6 categories, the percentage of perseverative errors ranged from 4.0% to 92.1%. More than two-thirds of the participants (69.5%) obtained less than 50% perseverative errors.
Pearson correlation coefficient was calculated for the relationship between MCST measures and demographic variables. For the percentage of perseverative errors, only

the 82 participants who completed fewer than 6 categories were analysed. There is a significant correlation between age and 4 MCST measurements: Cat, E, PE, and %PE. Education demonstrated a significant correlation in most of the MCST measurements except failure to maintain set (FinMS). Table 1 shows the correlation coefficient for age and education with each MCST measure.
To assess whether an individual participant’s Cat, E, and PE scores significantly differed from what might be expected given their age and education level, multiple regression equations were derived. The other MCST measures were excluded from this analysis since previous correlation analyses indicated that they had a low correlation with the predictor variables. Table 2 presents the regression coefficient for each case, together with the coefficient of multiple determinations.
As shown in Table 2, between 29% and 40% of the variance was accounted for by these equations. The partial correlation coefficients for both predictor variables were

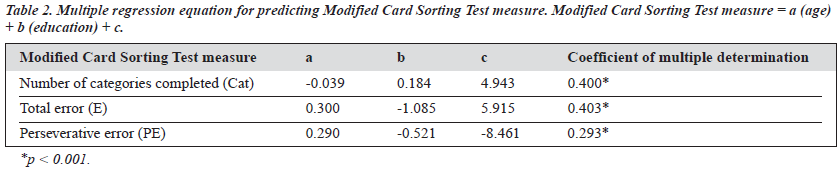
statistically significant (p < 0.05) in the equation of E and PE. However, the coefficient of age is non-significant in the equation of Cat. The variable age should therefore be neglected in the regression equation. In each case, education demonstrated a greater effect than age in the MCST measures.
Age Effect
The participants were further divided into 3 age groups as follows:
- pre-geriatric group — £65 years, n = 33
- young-old group — 66 to 75 years, n = 43
- older-geriatric group ³76 years, n = 19.
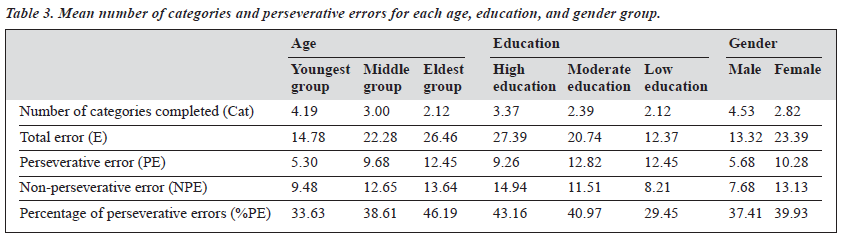
The group differences were analysed by ANOVA. There was significant group difference in Cat [F (2,94) = 9.39, p < 0.001], PE [F (2,94) = 8.392, p < 0.001], NPE [F (2,94) = 4.109, p < 0.05], and E [F (2, 94) = 10.638, p < 0.001]. Table 3 shows the means of each group. For Cat, E, and PE, the significant differences occur between the pre-geriatric group and both the young-old and older-geriatric groups, but not for the comparison between young-old and older-geriatric groups. For NPE, a significant difference only occurs in the compa- rison between the pre-geriatric and older-geriatric groups.
Education Effect
The participants were also divided into 3 education groups, as follows:
- low education — £2 years formal education, n = 27
- medium education — 3 to 9 years formal education, n = 40)
- high education — ³10 years formal education, n = 28.
The group differences were also analysed by ANOVA. Table 3 shows the mean in MCST measure for each group.
There was a significant group difference in Cat [F (2,94) = 16.152, p < 0.001], PE [F (2,94) = 8.838, p < 0.001], NPE [F (2,94) = 9.876, p < 0.05], E [F (2, 94) = 16.809, p < 0.001], and %PE [F (2,94) = 3.155, p < 0.05]. There were significant differences between all 3 education groups for Cat and E. For NPE, the low education group showed significant differences with the other 2 groups, while the difference between moderate and high education groups was non-significant. For PE, significant differences occurred between the high education group and both medium and low education groups. %PE showed significant differences between low and high education groups only.
Gender Difference
The 95 participants comprised 76 women and 19 men and gender differences in the MCST performances were analysed by t-test. There were significant differences in Cat (p < 0.001), PE (p < 0.05), NPE (p < 0.001), and E (p < 0.001). Table 3 shows the mean obtained by each gender group. On average, men obtained more categories and made fewer errors than women.
Discussion
This study recruited 95 community dwelling elderly participants with a wide educational range to perform the MCST. The results showed that approximately 86.3% of the healthy participants obtained 5 or fewer categories. This proportion appeared much higher than the 32.6%, 37.7%, and 43.0% reported in previous studies3,12,15 The relatively poorer performance in category completion may be related to excessive perseverative errors and/or non-perseverative errors. Since most errors made were non-perseverative, the unsuccessful completion of 6 categories was probably due to an inability to understand the nature and concepts of the task, or to remember previous responses. Another reason to account for the difference between the present and previous studies lies in the fact that, although previous studies also included older adults, most of the participants were younger, with a mean age of 40 to 53 years. Since the present study evaluated older people, with a mean age of 71.1 years, the fewer number of categories obtained may be explained by the declination of executive function in older adults. Further study in the comparison of MCST performance in different age groups should be conducted to address this hypothesis.
In the WCST, only a few people obtained no per- severative errors.1 In the present study, 5.3% of the healthy elderly people made no perseverative errors. The ability to achieve no perseverative errors in MCST can be explained by the fact that, in MCST, participants receive a warning that the sorting principle is going to change, while in WCST, participants learn the change of rule only after they have sorted the card correctly. Therefore, the first few sorts after the rule change is likely to be a perseverative error. In Nelson’s original study of MCST, a cut-off score of 50% perseverative errors was suggested to differentiate individuals with frontal lobe lesions from those without frontal lobe lesions, or from healthy individuals.3 Our study addressed the MCST performance of a community dwelling healthy elderly population, so comparison with the original study by Nelson was limited by a lack of people with frontal lobe lesions. However, in the present study, approximately 30% of participants received 50% or more perseverative errors. The results show the possibility of participants without neurological history to obtain a high proportion of perseverative errors, especially among elderly people. The large proportion of healthy elderly Chinese people receiving a score exceeding the cut-off score suggests that the performance of older adults is different to those results obtained in Nelson’s original report.3 A new cutoff score should be identified from future study to differentiate elderly people with frontal lobe lesions from healthy elderly people in the Chinese population.
Knowledge about factors that are associated with MCST performance not only help in the interpretation of an individual’s performance, but may also help in defining the cognitive mechanisms underlying MCST performance. Results from this present study also indicated that demo- graphic variables played a role in MCST performances. Age demonstrated significant influence on several MCST measures, including number of categories obtained and number of perseverative errors. The younger geriatric group performed better than their older counterparts. Performances declined with age, and people in the young-old group committed fewer perseverative errors than the older elderly age groups. Education also showed significant effects on many MCST measures, including number of categories obtained and number of perseverative errors.
In contrast to the age effect, education also demonstrated a significant effect on non-perseverative errors. The number of categories obtained decreases as the educational level decreases, and the high-education group obtained significantly fewer perseverative errors than other groups. This suggests that the high education group faced less difficulty and responded more flexibly to changes in the task. In order to investigate the contribution of age and education to MCST performances, multiple regression equations were done. Results show that education established a larger contribution than age in several MCST measures, including number of categories, total errors, and perseverative errors obtained.
Gender difference in MCST performances is subtle in previous studies. De Zubicaray et al indicated that gender has no effect on MCST performances,16 while Lineweaver et al found that men made significantly more non-perseverative errors than women.5 In the present study, however, gender illustrated a significant effect on MCST performances. Men achieved a better perfor- mance in the task and obtained more categories, fewer errors, and were less perseverative. Although these results appear to be different from previous findings, it should be noted that the number of men in the present study was much less than the number of women, and their education level was higher. Since education exerted an influence on MCST performances, the difference between men and women may not simply be due to the gender difference. Therefore, a larger number of men with a matched educational level should be recruited for further study of the gender effect.
The present study provided information about MCST performances of elderly Chinese people. Since age, education, and gender demonstrated influence on MCST performances, these demographic variables should be taken into account before MCST performances are interpreted. For the effective use of MCST as clinical assessment of neurological or psychiatric problems with elderly people, age- and education-based normative data should be developed.
References
- Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G. Wisconsin Card Sorting Test manual revised and expanded. USA: Psychological Assessment Resources, Inc; 1993.
- La Rue A. Aging and neuropsychological assessment. New York: Plenum Press; 1992.
- Nelson HE. A modified card sorting test sensitive to frontal lobe defects. Cortex 1976;12:313-324.
- Bondi MW, Monsch AU, Butters N, Salmon DP, Paulson JS. Utility of a modified version of the Wisconsin Card Sorting Test in the detection of dementia of the Alzheimer type. Clin Neuropsychol 1993;7:161-170.
- Lineweaver TT, Bondi MW, Thomas RG, Salmon DP. A normative study of Nelson’s (1976) Modified version of Wisconsin Card Sorting Test in healthy older adults. Clin Neuropsychol 1999;13:328-347.
- Korten AE, Henderson AS, Christensen H, et al. A prospective study of cognitive function in the elderly. Psycho Med 1997;27:919-930.
- Birren JE, Schaie KW. Handbook of the psychology of aging. San Diego: Academic Press; 2001.
- Krabbendam L, de Vugt ME, Derix MM, Jolles J. The behavioural assessment of the dysexecutive syndrome as a tool to assess executive functions in schizophrenia. Clin Neuropsychol 1999;13:370-375.
- Corcoran R, Upton D. A role of hippocampus in card sorting? Cortex 1993;29:293-304.
- Giovagnoli AR. Relation of sorting impairment to hippocampal damage in temporal lobe epilepsy. Neuropsychologia 2001;39:140-150.
- Traykov L, Baudic S, Thibaudet MC, Rigaud AS, Smagghe A, Boller
- F. Neuropsychological deficit in early subcortical vascular dementia: comparison to Alzheimer’s disease. Dement Geriatr Cogn Disord 2002;14:26-32.
- Van der Broek MD, Bradshaw CM, Szabadi E. Utility of the Modified Wisconsin Card Sorting Test in neuropsychological assessment. Br J Clin Psychol 1993;32:333-343.
- Lezak MD. Neuropsychological assessment. New York: Oxford University Press; 1995.
- De Zubicaray G, Ashton R. Nelson’s modified cards sorting test: a review. Clin Neuropsychol 1996;10:245-254.
- Obonsawin MC, Crawford JR, Page P, Chalmers P, Low G, Marsh P. Performance on the Modified Card Sorting Test by normal, healthy individuals: relationship to general intellectual ability and demographic variables. Br J Clin Psychol 1999;38:27-41.
- de Zubicaray GI, Smith GA, Chalk JB, Semple J. The Modified Card Sorting Test: test-retest stability and relationships with demographic variables in a healthy older adult sample. Br J Clin Psychol 1998;37: 457-466.
- Alexopoulos GS, Abrams RC, Young RC, Shamoian CA. Cornell Scale for depression in dementia. Biol Psychiatry 1988;23:271-284.
- Chiu HFK, Lee HC, Chung WS, Kwong PK. Reliability and validity of the Cantonese version of the Mini-Mental State Examination — a preliminary study. HK J Psych 1994;4 (Suppl 2):25-28.
