
Hong Kong J Psychiatry 2003;13(3):7-16
ORIGINAL ARTICLE
Abstract
Objective: To construct the Life Satisfaction Questionnaire.
Patients and Methods: Lehman’s ‘Quality of Life Interview Schedule’ was used as a template for the Life Satisfaction Questionnaire to measure levels of satisfaction in 9 life domains of young Chinese women with schizophrenia.
Results: Data obtained from 109 young Chinese women with schizophrenia were used to demon- strate the reliability of the instrument. Psychometric properties of the scale were found to be reliable and internally cohesive.
Conclusion: The Life Satisfaction Questionnaire was considered to be a potentially effective questionnaire for eliciting a woman’s satisfaction with her life. Further studies are needed to determine the questionnaire’s test-retest reliability and its generalisability to other groups of women with mental illness.
Key words: Chinese women, Life satisfaction, Mental illness, Questionnaire
Dr Tina Moyin Ng-Tse, PhD, Division of Health Sciences, Curtin University of Technology, Western Australia and School of Professional and Continuing Education, The University of Hong Kong, Hong Kong.
Address for correspondence:
Submitted: 22 March 2003; Accepted: 29 November 2003
Introduction
Life satisfaction or quality of life is an individual’s evaluation of the differences between his/her accomplishment and experiences as well as hopes and expectations at a particular period of time.1-2 Priorities, goals, and aspirations change with time and are modified by age and experience. There are 2 approaches to assess life satisfaction: subjective and objective. The method chosen is usually determined by the aims of the project. Often, both approaches are adopted by researchers. However, the estimate of distance between an individual’s position and his goals may vary depending on who makes the assessment.3
Studies have found that correlation of perceptions of quality of life between patients and physicians is poor.4-8 However, mental status may affect a person’s thinking and perception, which may lead to a tendency to overly express satisfaction or dissatisfaction with certain aspects of life. It is the person’s subjective evaluation of life and that should be accepted as a valid and true reflection of the person’s life experience during that period of life,9 and the credibility of self-rated quality of life by patients with schizophrenia has been demonstrated.10 Thus a greater weight should be given to the individual’s subjective feelings about the distance from his/her goals than to the judgement of an assessor.3
The importance of effectively engaging patients in obtaining accurate data on their overall condition (such as health problems and the interaction of internal and contex- tual factors) to formulate a comprehensive diagnostic pro- file has been acknowledged.11 Certainly, a culturally relevant, valid, and reliable measurement tool could facilitate the pro- cess of appraising a patient’s condition. Many studies have been conducted to investigate ‘quality of life’, ‘life satisfaction’, and ‘well-being’ of people with mental illness and the instruments used were specifically developed for their patients. However, there is a lack of a culturally rel- evant measurement tool to assess the level of life satisfac- tion of the female population, in particular, Asian women.
This study attempts to construct a culturally relevant, valid, and reliable questionnaire to measure the level of life satisfaction of Chinese women with schizophrenia, using Lehman’s ‘Quality of Life’ Interview Schedule12 (QOLIS) as a template.
Patients and Methods
The Modification
The QOLIS was chosen as the template for the questionnaire because it is a carefully designed, psychometrically adequate instrument constructed to assess perception of quality of life along several dimensions. According to Lehman, the overall purpose of the QOLIS was to assess the life circumstances of persons with chronic mental illnesses, both in term of what they actually do and experience (‘objective’ quality of life) and their feelings about these experiences (‘subjective’ quality of life).12 During the structured interviews, patients would be asked about the quality of their lives in 8 areas: living situation, family, social relations, leisure activities, work, finances, personal safety and legal problems, and health, and to rate their level of satisfaction on a scale of 1 (terrible) to 7 (delighted). General life satisfaction was also assessed. The reported internal consistency and test-retest reliability of the QOLIS for objective life conditions and life satisfaction ranges from 0.5 to 0.9.
The QOLIS was specifically designed for the Western psychiatric population whose education, psychosocial, cultural, and psychiatric background is different to those of Chinese women with schizophrenia. Therefore, it is essential to modify the content of the QOLIS to reflect the social context of this particular group of Chinese women. However, it was not the intent of the study to translate word-for-word and carry the exact connotation of the English version of Lehman’s QOLIS. During the re-structuring process, those relevant items to be included in the Life Satisfaction Ques- tionnaire (LSQ) were discussed with a group of bilingual people, including health professionals and and members of the general public who had no knowledge of psychiatry. Meticulous care was taken to ensure the Chinese words used were culturally sensitive and relevant to the local context.
Lehman recognised the need for modification of the QOLIS if it were to be used for a different client group.12 This author suggested that all the subjective QOLIS domains should be retained. However, the domain on ‘legal and safety’ was deemed not to be appropriate to the Chinese setting and was eliminated from the new questionnaire. Three new domains, namely, ‘managing problems’, ‘unemployment’, and ‘medication’, were added to the questionnaire as they were found to have great impact on a patient’s quality of life.13 In regard to the QOLIS, core objective indicators that have “the most universal appeal and have the best characterised psychometric properties and available norm”13 were retained except the one on ‘finances’. This was because of the different economic structure between the USA and Chinese societies.
Another major change to the QOLIS is the conversion of the data collection format from a structured interview schedule to a self-reporting questionnaire. In view of the education policy in the research sites — Hong Kong and Shenzhen, where education for all citizens is compulsory — the author has taken the liberty of assuming that all the women were literate. The assumption was confirmed after many interviews with female patients in hospitals and outpatient clinics. In fact, people in Hong Kong and Shenzhen have a tight time schedule and it would be impossible to engage them in a 1-hour structured interview. Therefore, reconstruction of the QOLIS to a self-reporting 7-point Likert scale questionnaire format was deemed desirable.
As a result of the modification, 1 subjective domain (legal and safety) and 1 objective indicator (finances) were eliminated from the QOLIS and 3 new subjective domains (unemployment, medication, and managing problems) were included.TheLSQ measuring life satisfaction of Chinese women with schizophrenia comprised 9 life domains (living situation, daily activities, social relations, family relations, health, finances, employment/unemployment, medication, and managing problems) and a general life satisfaction state- ment on which patients could express their degree of agreement on a separate 7-point scale, or yes-no format, where appropriate (Appendices 1 and 2 ). The point of discrimination between ‘satisfaction’ and ‘dissatisfaction’ of the questionnaire is made between the scores of 3 or 5. Therefore, a score of 4 or more is arbitrarily used as an indicator of satisfaction.
The Development Process
The essence of the interview questions of the QOLIS were captured and written as statements that formed the foundation of the questionnaire. Those items not relevant to Chinese social settings were eliminated. Additional items deemed important to the local culture, as judged by a panel of experts, were included. To ascertain clarity, readability, and unambiguity of the questionnaire, the draft version was given to 3 female inpatients to complete and they were asked for feedback on their understanding of the statements. Consequently, revisions and refinements were made to eliminate problems encountered during the consultation process. The edited version of the LSQ was reproduced for the final administration.
Patients
The study was conducted in the 2 psychiatric outpatient clinics on Hong Kong Island and the 1 clinic in Shenzhen. The probability sampling approach was used for the study because greater confidence could be placed on the representation of the target population.
Prospective participants were women aged 20 to 35 years residing in Hong Kong and Shenzhen with a history of schizophrenic illness for not less than 2 years and not more than 8 years and had no history of substance abuse or any neurological disease or physical illness which might affect their psychosocial functioning. Attempts were made to recruit all eligible participants attending the clinics in Hong Kong (n = 93) and Shenzhen (n = 56) to the study.
A total of 149 LSQs were hand-delivered to the eligible participants. Only 109 completed questionnaires were returned (68 from Hong Kong and 41 from Shenzhen) and the response rate was 81.5%. The majority of the patients (77%) had never married, 18% were married, and 5% were divorced. Only 65% of the women were employed, 27% were unemployed, and the rest were either engaged in full-time study or home duties. The majority of the women had received secondary school or post-secondary school education. Overall, the demographic data showed no significant differences between the 2 research sites, but the rate of unemployment was approximately 9-fold higher than the general population in Hong Kong and Shenzhen.
Statistical Procedures
The data were analysed using the Statistical Package for the Social Sciences computer program (Version 8 for Windows). The following procedures were used to analyse the psychometric properties of the LSQ.
Principal factors extraction method with Varimax rotation was employed to maximise relationships between variables. Multi-trait scaling analysis was used to confirm the unidimensionality of the sub-scale. Only those items showing item-total correlation between 0.3 and 0.7 would be included in further analysis. Further, Barlett Test of Sphericity should be significant and Kaiser-Myer-Olkin (KMO) measure of sampling adequacy should be greater than 0.6. Finally, Cronbach’s a coefficient of internal consistency (acceptable level was set in the vicinity of 0.6 to 0.7) was used to ensure that the items comprising each factor produced a reliable subscale.
Results
Table 1 summarises and compares the coefficient of the subjective domains between the LSQ and Lehman’s QOLIS. Details of the modified Life Satisfaction Questionnaire (LSQ) are as follows.
Living Situation
The original 3 QOLIS statements designed to elicit information regarding the patient’s living conditions were retained in the questionnaire (items 2 to 4). Standard procedures were followed to measure the reliability of this subscale. The results showed that the standardised a coefficient of this subscale (0.67) was considered to be satisfactory, but lower than the QOLIS (0.87). On closer examination of the items, it was found that one of the items “the prospect of staying on where you currently live for a long period of time” might not be relevant to the target group. This might be due to the fact that a woman, single or married, in a traditional Chinese environment is supposed to live with her family. In future, it would seem to be desirable to delete


Daily Activities
All of the 5 original QOLIS statements that assessed a subject’s satisfaction with leisure activities were retained (items 5 to 9). The a coefficient of the variable of both versions was the same (0.81). A list of 10 daily activities, classified under the headings of ‘social activity’, ‘non-social activity’, and ‘household activity’ (Table 2) was modified from the QOLIS in order to accurately measure the woman’s engagement in an average week. The subject would be asked to tick the activities she had done in the past week.
Social Relations
This variable attempted to explore the subject’s level of satisfaction with her general social interaction. In order to have a better knowledge of the woman’s relationship with her peers in terms of emotion and instrumental support, a subscale of 6 items, including 2 of the 3 QOLIS statements, was con- structed (items 17 to 22). Cronbach’s a coefficient of internal consistency ensured that the items comprising one single factor was a reliable scale (a = 0.83). Factor analysis also con- firmed a single factor represented by the 6 items (Table 3).
In addition to the 6 items exploring the subjective expe- rience with social relations, 3 descriptive items, in a form of 4-point Likert scale (at least once a day, at least once a week, at least once a month, and not at all), were included to elicit more information on frequency and modes of contact with friends (items 63 to 65).
Family Relations
The subjective and objective indicators of this variable aimed at exploring the relationship and frequency of contacts

between the woman and her family. In order to explore the level of satisfaction with family interaction, in addition to the original one of the 2 items, 2 new items were included (items 23 to 25). The reliability (0.80) of the modified subscale was satisfactory. Similar to the structure of the objective domain of the social relation, 2 items were included to explore the frequency of contact and togetherness as a family (items 61 to 62).
Health
This variable aimed to measure a woman’s satisfaction with her physical and emotional health. The notion that people with chronic illness tend to compare their own health status with people who are in a worse situation has been acknowledged. Therefore, in addition to the 3 QOLIS statements, a new item that was used to explore the patient’s satisfaction with her health status when compared with others was included (items 39 to 42). Reliability of the modified subscale was 0.80. Further to the 4 items on a 7-point subscale for measuring satisfaction of general health, another 4 true-false statements from the QOLIS were included in the questionnaire (items 35 to 38).
Finances
This variable attempted to identify a woman’s level of satisfaction with her financial situation. All 3 QOLIS statements were retained (items 26 to 28) and the a coeffi- cient was found to be the same (0.87).
Employment
This subscale was designed to assess a woman’s satisfaction with her working conditions; that is, the people she worked with, the physical environment, and the salary (items 29 to 31). The reliability of the subscale, comprising 1 new item and 2 of the 3 original items, was 0.69.
Unemployment
Since not every woman has a job, this new sub-scale was constructed to explore the women’s perception of being unemployed (items 32 to 34). The inter-scale correlations solution showed the correlation of each item was acceptable (>0.40). The internal consistency of the variable was satisfactory (a = 0.65). It was found that the solution could not be rotated and the factor analysis indicated that only 1 component was extracted.
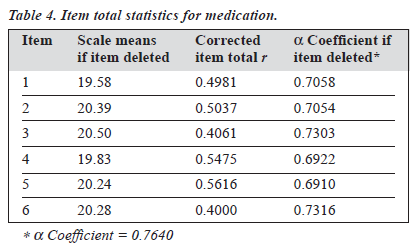
Medication
This new subscale was operationalised by 6 items in an attempt to explore a woman’s satisfaction with the treatment effect and side effects of medication (items 43 to 48). The a coefficient of the subscale was 0.76. The inter-scale correlations solution showed that the correlation of each item was satisfactory (Table 4).
A principal component factor analysis with Varimax rotation of 107 patients (2 of the pateints were not taking medication) resulted in 2 factors identifying that factor I (Q1, Q4, Q2) had an eigenvalue of 2, whereas factor II (Q3,

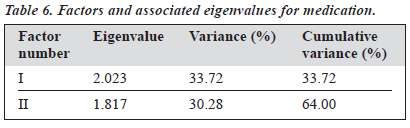
Q5, Q6) had a value of 1.8 (Table 5). These 2 factors accounted for 33.7% and 30.3% of total variance (Table 6). Factor I focused on the effectiveness of medication for main- taining health, while factor II emphasised the unpleasant side effects of medication.
In addition to the 6 items on a 7-point subscale for measuring the satisfaction with treatment effects, another set of 7 items in the form of a ‘yes-no’ response was con- structed to identify a woman’s opinions of the prescribed medication and her willingness for medication compliance (items 49 to 55). The data obtained from these items should provide more descriptive information about the effects of medication on a woman’s assessment of her wellbeing.
Managing Problems
The new subscale consisted of 6 items. Effects of problems on a woman’s life and ways of handling problems were presented by the items 10 to 16. Internal consistency for the variable was examined using Cronbach’s a. It was found that the item correlations were above 0.40. The a coeffi- cient was 0.77, which was considered to be satisfactory for a new scale (Table 7).
A varimax rotation based on the 6 items accounted for 64% of the total variance, with factor I contributing 33.6% and factor II contributing 30.1% (Table 8).
The 3 items on factor I related to the level of satisfac- tion with handling of problems. The 3 items for factor II



were concerned with the effect problems had on the person’s life (Table 9).
To understand the measures a woman uses to cope with problems, 8 different types of coping methods used by an average person were listed (item 56). The patient was asked to indicate the methods she would have employed in coping with stress or problems. A further 4 questions from the QOLIS were included to elicit information about sources of comfort that were available to the woman when she was confronted by problems (items 57 to 60).
Discussion
One of the objectives of providing good quality health care is to assist patients in achieving harmony with their internal and external environment. To this end, a large number of Western studies have been conducted using tailor-made in- struments for the target population to investigate the per- ceptions of people with mental illness and how it relates to their lives. In view of the lack of a culturally relevant mea- surement tool that can reflect the perceived levels of life satisfaction of Chinese women with schizophrenia, a self- completed Life Satisfaction Questionnaire (LSQ) using Lehman’s Quality of Life Interview Schedule (QOLIS) as a template was constructed. The LSQ comprises 9 life domains (living situation, daily activities, social relations, family relations, health, finances, employment/unemployment, medication, and managing problems), and patients can express their degree of agreement on a separate 7-point scale, or yes-no format, where appropriate.
The principal components analyses found that each do- main appeared theoretically relevant to the Chinese culture and psychosocially relevant to young Chinese women with mental illness. In terms of psychometric properties, adequate variance in scores was demonstrated. With respect to future use of the variables ‘living situation’ and ‘employment’, it would be beneficial to construct a few more linking items to cover a wider perimeter of the underlying construct. As predicted by the Spearman-Brown formula, there would be a moderate increase in test length contemplated and the a coefficient would substantially increase.
One of the significant contributions of the LSQ to the understanding of the respondents’ levels of life satisfaction is the inclusion of the respondents’ views of their state of health and perception of the effectiveness of pharmaceuti- cal interventions. Data collected from these domains would provide health professionals with a better idea of their cli- ents’ reactions to the effectiveness and side effects of medication, and provide intervention accordingly. This ap- proach would certainly enhance and compliment the human- istic approach to medicine.13
It has been argued that people in a disadvantaged situa- tion might lower their level of aspiration to narrow the gap between their achievements and aspirations.14 To maintain the optimal level of achievement, which in turn leads to a satis- factory level of quality of life, rehabilitation programmes for people with mental illness have been developed to address skill deficits in areas such as interpersonal relationship, occupation, and problem management. The domain of ‘manag- ing problems’ of the LSQ could provide health professionals a comprehensive overview on ways their clients manage problems encountered in everyday life and to design a tailor- made therapeutic intervention program to address their needs.
Methodological difficulties associated with measuring quality of life in the field of psychiatry have been ac- knowledged. Some of the problems highlighted are low reliability in relation to deficits in attention, comprehension, and motivation and low sensitivity due to emotional dull- ness and apathy.15,16 Despite the considerable amount of in- struments measuring life satisfaction, including this newly constructed LSQ, psychiatrists have yet to find one that can overcome the practical problems.
The content of the LSQ is not particularly female gen- der specific, except for those items under the domains of ‘daily activities’ and ‘managing problems’. Even so, many Chinese men are becoming more active in performing domestic chores. In view of this, the questionnaire would be more applicable to the male population if more male- oriented items were included.
At the time the LSQ was developed, it was considered to be a potentially effective questionnaire for eliciting a woman’s satisfaction with her life. However, the study only involved 109 Chinese women with schizophrenia. Further studies are needed to determine the questionnaire’s test- retest reliability and its generalisability to other groups of women with mental illness.
References
- Calman K. Definitions and dimension of quality of life. In: Aaronson N, Beckmann J, editors. The quality of life of cancer patients. New York: Raven Press; 1987.
- Saxena S, Orley J. Quality of life assessment: the World Health Organization perspective. Eur Psychiatry 1997;12 (Suppl. 3):263-266.
- Sartorius N. Cross cultural comparisons of data about quality of life: a sample of issues. In: Aaronson N, Beckmann J, editors. The quality of life of cancer patients. New York: Raven Press; 1987.
- Fitzgerald PB, Williams N, Corteling SL, et al. Subject and observer- rated quality of life in schizophrenia. Acta Psychiatr Scand 2001;103: 387-391.
- Koivumaa-Honkanen HT, Honkanen R, Antikainen R, Hintkkka J, Viinamaki H. Self-report life satisfaction and treatment factors in patients with schizophrenia, major depression and anxiety disorder. Acta Psychiatr Scand 1999;99:377-384.
- Sainfort F, Becker M, Diamond R. Judgements of quality of life of individuals with severe mental disorders: patient self-report versus provider perspectives. Am J Psychiatry 1996;153:497-502.
- Slevin MR, Plant H, Drinkwater J, Gregory WM. Who should measure quality of life, the doctor or the patient? Br J Cancer 1988;57:109-112.
- Trauer T, Duckmanton RA, Chiu E. A study of the quality of life of the severely mentally ill. Int J Soc Psychiatry 1998;44:79-91.
- Orley J, Saxena S, Herrman H. Quality of life and mental illness: re- flections from the perspective of WHOQOL [editorial]. Br J Psychiatry 1998;172:291-293.
- Van Dongen C. Quality of life and self esteem in working and non- working persons with mental illness. Community Ment Health J 1996; 32:535-548.
- IGDA Working Group, WPA. IDGA. 1: Conceptual bases — historical, cultural and clinical perspectives. Br J Psychiatry 2001;182 (Suppl 45): 40-41.
- Lehman A. Quality of life manual. USA: University of Maryland; 1991.
- Ng-Tse T. Factors associated with the successful community placement of the chronic mentally ill. Proceedings of Australia’s First International Psychiatric Nursing Conference; Australia: Melbourne 1994, July:61-70.
- Lomachenkov AS. Quality of life of patients and assessment of therapeutic medical interventions. Int J Ment Health 2002;31:1, 13-18.
- Katschnig H. Schizophrenia and quality of life. Acta Psychiatr Scand Suppl 2000;102(407):33-37.
- Burkovskii GV, Kabanov MM, Kotsiubinskii AP, et al. Methods and problems in developing and using instruments for measuring the quality of life of the mentally ill. Int J Ment Health 2002;31:1, 49-61.
