
East Asian Arch Psychiatry 2018;28:17-22
ORIGINAL ARTICLE
Dr Ambrish S Dharmadhikari, DNB (Psychiatry), Senior Resident, Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India.
Prof Avinash L Tandle, MTech, Assistant Professor, Department of Electronics & Telecommunication, Mukesh Patel School of Technology, Management & Engineering, NMIMS University, Mumbai, Maharashtra, India.
Dr Suyog V Jaiswal, MD (Psychiatry) Assistant Professor, Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India.
Dr Vishal A Sawant, MD (Psychiatry), Honorary Psychiatrist, Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India.
Dr Vihang N Vahia, MD (Psychiatry), Professor Emeritus, Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India.
Dr Nandini Jog, PhD, Professor, Department of Electronics & Telecommunication, Mukesh Patel School of Technology, Management & Engineering, NMIMS University, Mumbai, Maharashtra, India.
Address for correspondence: Dr Suyog V Jaiswal, Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India. Email: suyogjaiswal@gmail.com
Submitted: 18 January 2017; Accepted: 7 November 2017
Abstract
Introduction: Electroencephalography (EEG) has been used extensively to study affective disorders. Quantitative spectral analysis of an EEG scan has been used to assess the biological basis of emotional disorders such as depression as well as to investigate biomarkers of affective disorders. Inter-hemispheric asymmetries in both baseline and stimulus-evoked frequencies (alpha, beta, theta, and delta) are potential biomarkers of depression. The role of frontal alpha asymmetry has been established, but other spectral frequencies such as frontal theta remain elusive. We compared the hemispheric differences in frontal theta power in depressed patients and controls before and during listening to music to study the correlation of frontal theta asymmetry with depression.
Methods: To determine whether stimulus-evoked frontal theta asymmetry is a biomarker of depression, we compared 23 patients with mild depression (based on the Hamilton Depression Rating Scale) with 17 age- and sex-matched controls by conducting EEG at rest and after listening to Indian classical music.
Results: In controls without depression, the mean frontal theta power of the left hemisphere and frontal theta asymmetry increased significantly during music listening. In depressed patients, frontal theta asymmetry was reversed during music listening.
Conclusion: Frontal theta asymmetry is a potential biomarker of depression.
Key words: Depression; Electroencephalography; Music
Introduction
Depression is a common illness worldwide, with an estimated 350 million people affected. It is a major cause of disability and a major contributor to the global disease burden.1 It is associated with attention and memory difficulties. When depressed, individuals engage fewer processes that require attention,2 and invariably complain of concentration and memory problems.3
Quantitative electroencephalography (EEG) is a non-invasive neuro-electric tool that is used to study the biological basis of depression. Among spectrally analysed frequencies, alpha (8-13 Hz) asymmetry has received most attention.4 Beta (13-28 Hz),5 theta (5-7 Hz), and delta (1-4 Hz)6,7 asymmetry are potential biomarkers for depression, making hemispheric differences in frequencies the main theme of depression study.
The hippocampus has been hypothesised to be the anatomical origin of depression, with a lower volume in depressed subjects.8 It is the predominant source of theta waves in the frontal lobe.9 Research on theta spectral frequency has focused on changes in frontal midline theta frequency and their correlation with anxiety rather than depression.10 There is no evidence yet to support frontal theta asymmetry as a biomarker of depression. Nonetheless, frontal theta changes seem to be indicative of the emotional processing of music, as frontal theta power increases in EEG during listening to pleasant music.11 There is hemispherically differential processing of emotion: positive emotions are related to a preponderance of left frontal activation, whereas negative emotions result in a more bilateral frontotemporal activation, with dominance of the right hemisphere.12
Music is a powerful elicitor of emotion.13-15 Musicologists believe that the essence of music lies in the emotions that they describe or invoke.16-18 Music is used in various cultures to express and inspire emotions, from declaring love to lamenting the death of a loved one and inspiring patriotic and military action.19 Central processing of musical stimuli has focused primarily on cognitive aspects Behavioural tendencies of approach and withdrawal are postulated to be due to differential processing of the left and right frontal lobes, respectively.22
We thus compared the hemispheric differences in frontal theta power in depressed patients and in matched controls before and during listening to Indian classical music to examine the correlation between frontal theta asymmetry and depression.
Methods
Study Design
This case-control study was approved by the ethics committee of our institution. Written informed consent was obtained from each participant. Cases were consecutive patients from a psychiatry out-patient department of a tertiary-care public hospital in urban India during a period of 3 months (August 2015 to October 2015). A total of 23 patients who were diagnosed with a depressive episode (F32; ICD-10)23 of mild severity (Hamilton Depression Rating Scale score of 8 to 13)24 were included. They were prescribed a selective serotonin reuptake inhibitor, preferably escitalopram. Patients who were prescribed any mood stabiliser or benzodiazepine as part of their antidepressant regimen were excluded, as were those with comorbid substance use, anxiety disorder, or other psychiatric, physical, or neurological illness. In addition, 23 age- and sex-matched volunteer controls (relatives of patients from other departments, medical students, and hospital staff) were recruited after explaining the study and obtaining written informed consent; data in 6 controls were rejected owing to excessive EEG artefacts. Those with physical or neurological disease or a history of depression based on an interview, or any current diagnosable psychiatric condition apart from depression based on the Mini-International Neuropsychiatric Interview25 were excluded. Both cases and controls had no formal training in music; all had right- hand dominance according to the Edinburgh Handedness Inventory.26
Musical Stimulus
One of the characteristics of Indian classical music is the allocation of distinct times of the day and night for playing Raga melodies. It is believed that only during this period do ragas reach the height of their melodic beauty and majestic splendour. Raag Bhairavi is an early morning raga and is performed as a concluding piece of music at every concert. Its melodic sequences can cover all the 12 notes of the scale (as pure, hard, and soft notes) with skill. Soft notes (Komal) are below the fundamental frequency and hard notes (Teevra) are above. The notes in the Raag Bhairaviare are Sa, Re(S), Re, Ga(S), Ga, M, M(H), Pa, Dha(S), Dha, Ni(S), and Ni. The soft notes and their smooth rendering are said to have pleasing and fulfilling effects on the listener. Musical instruments of Raag Bhairavi include the flute, jaltarang, santoor, and harmonium.27,28 In this study, each participant was played one version in which the musical instrument was randomly selected.
Data Acquisition
To evaluate brain activity, an electrode cap of 19 electrodes was placed on the scalp based on the international 10-20 system and connected to a 32-channel EEG machine. A noise-cancelling headset was used to deliver the stimulus for 10 minutes, and EEG was recorded in a soundproof laboratory in dim light, including a period of 10 minutes before and after the stimulus. Participants were asked to rate the emotions evoked by the music on a visual analogue scale of 0 to 5. A score of 0 was extremely negative or unpleasant emotions and a score of 5 was extremely positive or pleasant emotions. All artefacts other than electro-oculography were removed manually.29 To minimise electro-oculographic and physiological artefacts, participants were instructed to close their eyes and avoid eye movement. All muscle, ocular, and movement artefacts of EEG signals and rejected offline EEG signals were recorded with a sampling rate of 256 Hz; x (n), with n = 0, 1, 2, 3…. N-1 being the raw sample of EEG at the frontal side. Artefact-free EEG signals were epoched with a Hanning window.30
Equation 1 represents the fast Fourier transform algorithm for the theta band after applying a Hanning window (Xθ = Fourier transform, H(n) = Hann window, and x(n) = raw EEG score). In Equation 2, (TFθPL)BD denotes total frontal theta power in the left frontal lobe (at electrode Fp1-A1, F7-A1, and F3-A1) before and during music listening. In Equation 3, (TFθPL)BD denotes total frontal theta power in the right frontal lobe (at electrode Fp2-A2, F8-A2 and F4-A2) before and during music listening.
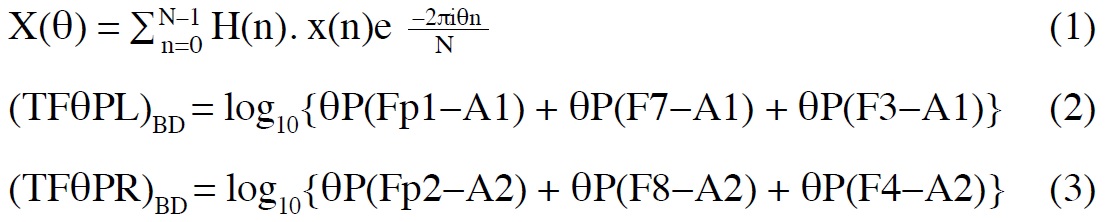
The mean power for the theta band across all frontal electrodes was calculated. Data were normalised by log transformation in equations 1 to 3 using NeuroMax 3.0.01 software.31 Statistical analysis was performed using an open source software R 3.4.1.32 The one-way analysis of variance (ANOVA), paired t-test, Tukey test, or Kruskal-Wallis test was used, as appropriate. A p value of <0.05 was considered statistically significant.
Results
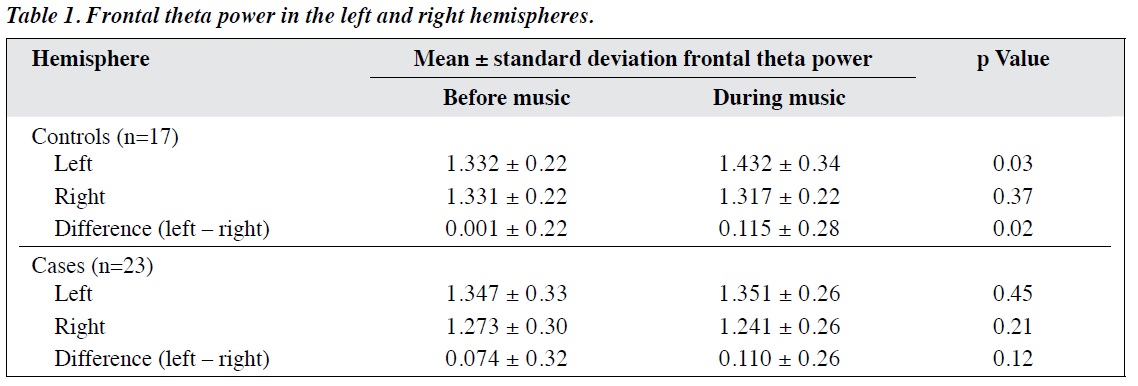
The mean ± standard deviation age of the controls without depression was 29.5 ± 9.8 years and that of the patients with depression was 34.8 ± 11.1 years. In the control group, the mean frontal theta power of the left hemisphere increased significantly during music listening. The difference in mean frontal theta power between the left and right hemispheres (frontal theta asymmetry) also increased significantly during music listening (Table 1). In the group of depressed patients, there was no significant increase in the mean frontal theta power or frontal theta asymmetry during music listening.
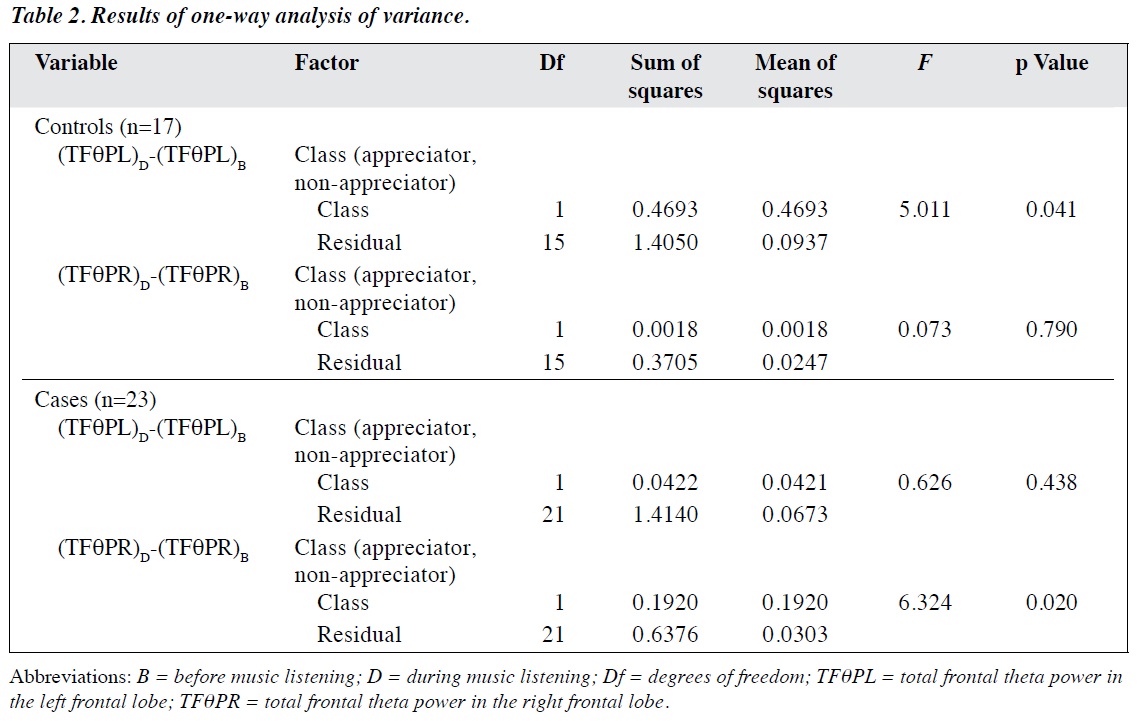
One-way ANOVA was used to compare appreciators with non-appreciators, according to the emotions evoked by the music on a visual analogue scale. In the controls, the total frontal theta power during music listening increased significantly in the left hemisphere (F (1, 15) = 5.011; p = 0.041), but the difference in the right hemisphere was not significant (F (1, 15) = 0.073; p = 0.790). In the depressed patients, the total frontal theta power during music listening decreased significantly in the right hemisphere (F (1, 21) = 6.324; p = 0.020), but the difference in the left hemisphere was not significant (F (1, 21) = 0.626; p = 0.438) [Table 2].
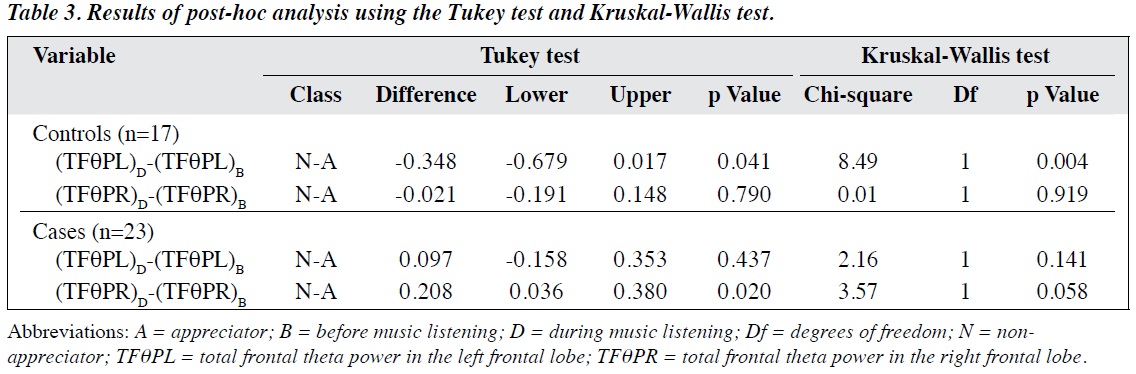
Post-hoc comparison was made using the Tukey test and Kruskal-Wallis test. In the Tukey test, during music listening among the controls, the left hemisphere theta power increased significantly (p = 0.041) but the difference in the right hemisphere was not significant (p = 0.790). In contrast, among the depressed patients, the right
hemisphere theta power decreased significantly (p = 0.020) but the difference in the left hemisphere was not significant (p = 0.437). In the Kruskal-Wallis test, the increase in the left hemisphere theta power in controls remained significant (p = 0.004), but the reduction in the right hemisphere theta power in patients was barely non-significant (p = 0.058) [Table 3].
Discussion
Frontal theta asymmetry is a potential biomarker for depression, but the evidence is primarily based on animal studies and emotion theory analysis.33,34 The asymmetry depends on the severity of depression: the more severe the depression is, the greater the reduction is in the evoked frontal theta power secondary to stimuli.35 Nonetheless, it is difficult to differentiate between a normal population and mildly depressed patients. This study aimed to assess frontal theta changes in patients with mild depression.
We used Indian classical music as the stimulus to evoke EEG changes across the frontal region, with a focus on theta waves. Most studies have reported that during music listening, the alpha and theta power of the left anterior hemisphere increases; in particular, there are significant theta power changes in the left anterior region, representing activity in Brodman areas 44, 45, 46, 47, and 38.36 In our control group, the frontal theta power of the left hemisphere increased significantly during music listening. This result formed the benchmark for comparison with depressed patients, in whom frontal theta asymmetry did not change significantly (Table 1). Hemispherically differential processing of music in normal subjects37 was also previously evident in patients with depression. It was interesting to observe that frontal theta asymmetry reversed in patients with depression; even those who appreciated music still processed music with the right hemisphere.
Anatomical correlation studies using EEG support the evidence of frontal theta power in depression. An increase in theta power in the mid-frontal areas is associated with cerebral metabolic changes in the anterior cingulate cortex.38 In depressed patients, an increase in theta power is associated with dipole activity in the middle cingulate cortex that is induced by music with emotional valence and arousal.39 Frontal theta power increases significantly after 22 seconds of listening to pleasant music.40
In our study, the resting EEG showed a focus of attention on music that followed. Functional increases of power and coherence in the theta frequency range are indicators of internal creative cognitive associations that “arise from integration through the co-activation by slow wave activity of distributed neural networks”.41 In our study, differences in lateralisation and power indicated that the controls learned to relax and focused their attention on internal processes; this effect was not seen in patients with depression. Frontal theta asymmetry can be a biomarker of depression, as there is evidence of impaired sustained attention in patients with mild depression, although this has also been found in patients with anxiety and other psychiatric illness.42 In our study, we made efforts to select patients with mild depression only.
Some studies have used objective factors such as EEG-based measures43,44 and non-EEG physiological variables46 with or without psychological tests to assess or predict clinical change in patients. Other studies have relied on subjective assessments alone.47,48 In our study, EEG- based measures were used as outcome measures. In addition to clinical evaluations based on human judgement, EEG- based measures such as frontal theta asymmetry and frontal alpha asymmetry may be used as biomarkers of depression, particularly when expertise is inadequate. Given that mental functioning is a complex phenomenon, EEG-based measures might aid in diagnosis in addition to established psychiatric assessments. Further research is needed to investigate the correlation of potential biomarkers for depression with the established findings. Both frontal alpha asymmetry and frontal theta asymmetry have an empirical basis to support their use. It might be that certain aspects of depression and anxiety are closely related to frontal alpha asymmetry and frontal theta asymmetry.
This study had some limitations. The sample was
small and thus generalisable only to a clinically referred population rather than the general population. For example, the high proportion of women may have reflected a higher prevalence of depression in women or a greater readiness of women to seek treatment. The effect of the course of depression on EEG changes was not known. Our patients with depression were prescribed selective serotonin reuptake inhibitors, although in theory the antidepressant does not interfere with frontal theta power. In addition, depression was not differentiated as reactive, endogenous, or familial. A genetic predisposition to depression or early neuronal changes that lead to depression could not be excluded. Future studies may use frontal theta asymmetry as a biomarker to assess treatment response in patients with depression.
Conclusion
Frontal theta asymmetry is a potential biomarker of depression, as is frontal alpha asymmetry and frontal midline theta power.
Acknowledgements
We thank Dr Deoraj Sinha from the Department of Psychiatry, H B T Medical College & Dr R N Cooper Municipal General Hospital, Mumbai, Maharashtra, India, for his contribution to the study.
Declaration
The authors have no conflicts of interest to disclose.
References
- World Health Organization. Media Centre. Depression. Available from: http://www.who.int/mediacentre/factsheets/fs369/en/.Accessed on 8 Dec 2016.
- Hartlage S, Alloy LB, Vázquez C, Dykman B. Automatic and effortful processing in depression. Psychol Bull 1993;113:247-78. cross ref
- Kahn RL, Zarit SH, Hilbert NM, Niederehe G. Memory complaint and impairment in the aged. The effect of depression and altered brain function. Arch Gen Psychiatry 1975;32:1569-73. cross ref
- Knott V, Mahoney C, Kennedy S, Evans K. EEG power, frequency, asymmetry and coherence in male depression. Psychiatry Res 2001;106:123-40. cross ref
- Pollock VE, Schneider LS. Quantitative, waking EEG research on depression. Biol Psychiatry 1990;27:757-80. crossref
- Knott VJ, Lapierre YD. Computerized EEG correlates of depression and antidepressant treatment. Prog Neuropsychopharmacol Biol Psychiatry 1987;11:213-21. cross ref
- Kwon JS, Youn T, Jung HY. Right hemisphere abnormalities in major depression: quantitative electroencephalographic findings before and after treatment. J Affect Disord 1996;40:169-73. cross ref
- Maletic V, Robinson M, Oakes T, Iyengar S, Ball SG, Russell J. Neurobiology of depression: an integrated view of key findings. Int Clin Pract 2007;61:2030-40. cross ref
- Klimesch W. EEG alpha and theta oscillations reflect cognitive and memory performance: a review and analysis. Brain Res Brain Res Rev 1999;29:169-95. cross ref
- Schacter DL. EEG theta waves and psychological phenomena: a review and analysis. Biol Psychol 1977;5:47-82. cross ref
- 1 Sammler D, Grigutsch M, Fritz T, Koelsch S. Music and emotion: electrophysiological correlates of the processing of pleasant and unpleasant music. Psychophysiology 2007;44:293-304. crossref
- Altenmüller E, Schürmann K, Lim VK, Parlitz D. Hits to the left, flops to the right: different emotions during listening to music are reflected in cortical lateralisation patterns. Neuropsychologia 2002;40:2242-56. crossref
- Goldstein A. Thrills in response to music and other stimuli. Physiol Psychol 1980;8:126-9. cross ref
- Panksepp J. The emotional sources of “chills” induced by music. Music Percept 1995;13:171-207. cross ref
- Sloboda JA. Music structure and emotional response: some empirical findings. Psychol Music 1991;19:110-20. cross ref
- Cooke D. The Language of Music. London: Oxford University Press; 1959.
- Langer SK. Philosophy in a new key. A Study in the Symbolism of Reason, Rite, and Art. Cambridge: Harvard University Press; 1959.
- Meyer LB. Emotion and Meaning in Music. Chicago: University of Chicago Press; 1956.
- Trehub SE, Trainor L. Singing to infants: lullabies and play songs. Adv Infancy Res 1998;12:43-77.
- Samson S, Zatorre RJ. Learning and retention of melodic and verbal information after unilateral temporal lobectomy. Neuropsychologia 1992;30:815-26. cross ref
- Trainor LJ, Desjardins RN, Rockel C. A comparison of contour and interval processing in musicians and nonmusicians using even-related potentials. Aust J Psychol 1999;51:147-53. crossref
- Davidson RJ, Schwartz GE, Saron C, Bennett J, Goleman DJ. Frontal versus parietal EEG asymmetry during positive and negative affect. Psychophysiology 1979;16:202-3.
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems. Geneva: World Health Organization; 2004.
- Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960;23:56-62. cross ref
- van Vliet IM, de Beurs E. The MINI-International Neuropsychiatric Interview. A brief structured diagnostic psychiatric interview for DSM-IV en ICD-10 psychiatric disorders [in Dutch]. Tijdschr Psychiatr 2007;49:393-7.
- Caplan B, Mendoza JE. Edinburgh handedness inventory. In: Encyclopedia of Clinical Neuropsychology. New York: Springer; 2011: 928. cross ref
- Raag Bhairavi. Available from: http://www.tanarang.com/english/bhairavi_eng.htm. Accessed 30 Jul 2015.
- Tandle A, Jog N, Dharmadhikari A, Jaiswal S, Sawant V. Study of valence of musical emotions and its laterality evoked by instrumental Indian classical music: an EEG study. 2016 International Conference on Communication and Signal Processing (ICCSP). crossref
- Tandle A, Jog N, D’cunha P, Chheta M. Classification of artefacts in EEG signal recordings and EOG artefact removal using EOG subtraction. Commun Appl Electron 2016;4:12-9. crossref
- Tandle A, Jog N, Dharmadhikari A, Jaiswal S. Estimation of valence of emotion from musically stimulated EEG using frontal theta asymmetry. 12th International Conference on Natural Computation, Fuzzy Systems and Knowledge Discovery (ICNC-FSKD). 2016;63-8. crossref
- NeuroMax Released 2014. Version 3.0.01. Chandigarh: Medicaid System Inc. Available from: http://www.medicaid.co.in. Accessed 11 Oct 2016.
- R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available from: http://www.R-project.org/. Accessed 11 Oct 2016.
- Dandawate YH, Kumari P, Bidkar A. Indian instrumental music: raga analysis and classification. 1st International Conference on Next Generation Computing Technologies (NGCT). 2015:725-9. cross ref
- Harmon-Jones E, Gable PA, Peterson CK. The role of asymmetric frontal cortical activity in emotion-related phenomena: a review and update. Biol Psychol 2010;84:451-62. cross ref
- Mitchell DJ, McNaughton N, Flanagan D, Kirk IJ. Frontal-midline theta from the perspective of hippocampal “theta”. Prog Neurobiol 2008;86:156-85. cross ref
- Gold C, Fachner J, Erkkilä J. Validity and reliability of electroencephalographic frontal alpha asymmetry and frontal midline theta as biomarkers for depression. Scand J Psychol 2013;54:118-26. crossref
- Thatcher RW, Biver C, North D. 2009 Neuroguide (version 2.5.6). St Petersburg. Available from http://www.appliedneuroscience.com. Accessed 24 Nov 2016.
- Pizzagalli DA, Oakes TR, Davidson RJ. Coupling of theta activity and glucose metabolism in the human rostral anterior cingulate cortex: an EEG/PET study of normal and depressed subjects. Psychophysiology 2003;40:939-49. cross ref
- Lin YP, Duann JR, Chen JH, Jung TP. Electroencephalographic dynamics of musical emotion perception revealed by independent spectral components. Neuroreport 2010;21:410-5. crossref
- Sammler D, Grigutsch M, Fritz T, Koelsch S. Music and emotion: electrophysiological correlates of the processing of pleasant and unpleasant music. Psychophysiology 2007;44:293-304. crossref
- Gruzelier J. A theory of alpha/theta neurofeedback, creative performance enhancement, long distance functional connectivity and psychological integration. Cogn Process 2009;10(Suppl 1):S101-9. crossref
- Leuchter AF, Cook IA, Hunter AM, Cai C, Horvath S. Resting- state quantitative electroencephalography reveals increased neurophysiologic connectivity in depression. PLoS One 2012;7:e32508. cross ref
- Fachner J, Gold C, Erkkilä J. Music therapy modulates fronto-temporal activity in rest-EEG in depressed clients. Brain Topogr 2013;26:338-54. crossref
- O’Kelly J, Magee WL. Music therapy with disorders of consciousness and neuroscience: the need for dialogue. Nord J Music Ther 2013;22:93-106. cross ref
- Haslbeck FB. Music therapy for premature infants and their parents: an integrative review. Nord J Music Ther 2012;21:203-26. crossref
- Teckenberg-Jansson P, Huotilainen M, Pölkki T, Lipsanen J, Järvenpää AL. Rapid effects of neonatal music therapy combined with kangaroo care on prematurely-born infants. Nord J Music Ther 2011;20:22-42. crossref
- Albornoz Y. The effects of group improvisational music therapy on depression in adolescents and adults with substance abuse: a randomized controlled trial. Nord J Music Ther 2011;20:208-24. crossref
- Gattino GS, Riesgo RD, Longo D, Leite JC, Faccini LS. Effects of relational music therapy on communication of children with autism: a randomized controlled study. Nord J Music Ther 2011;20:142-54. crossref
